Материал: BASIC CLINICAL SYNDROMES IN INTERNAL DESEASES CLINIC
With decompensation - weakness, dizziness, fainting, heart pain, angina pectoris;
Inspection - pallor of the skin, visible mucous membranes, increased apical impulse;
Palpation: the apical impulse is displaced to the left, diffuse, resistant, high, ―raising‖, systolic trembling (―cat purr‖) in the second intercostal space to the right of the sternum - palpation analogue of systolic murmur;
Percussion - an increase in the left border of relative dullness, an expansion of vascular dullness in the second intercostal space to the right (post-stenotic expansion of the ascending aorta);
Auscultation: I tone at the apex is weakened, II tone at the aorta is weakened, gross systolic murmur on the aorta (maximum point), which is carried out on the carotid arteries and in the interscapular region, often above the entire surface of the heart, is better heard in a horizontal position on the exhale;
Pulse slow (pulsus parvus), rare (pulsus rarus), small (pulsus tardus), systolic and pulse blood pressure decreased;
ECG: signs of severe left ventricular hypertrophy;
FCG: consistent with auscultatory picture;
Echocardiography: reducing the amplitude of systolic opening, thickening, limiting the mobility of the valves of the aortic valve. Hypertrophy of the left ventricular myocardium, a decrease in the area of the aortic opening, dilatation of the ascending aorta (post-stenotic expansion) are clearly visible;
X-ray: "aortic" configuration of the heart due to concentric hypertrophy of the left ventricle. Often you can see calcification of the aortic valve, expansion of the initial part of the aorta;
Doppler echocardiography: a significant increase in the maximum velocity of blood flow through the mouth of the aorta.
With mitralization of the defect (the development of relative mitral valve insufficiency due to
dilatation of the left ventricle and expansion of the mitral orifice), it is possible to expand the borders of the heart to the right, due to hypertrophy of the right ventricle of the heart.
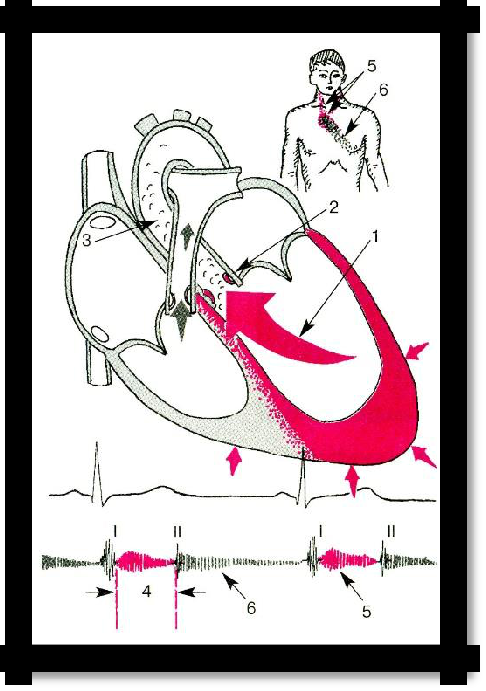
Pic 3.24 Aortic stenosis (hemodynamics).
46
Aortic valve insufficiency
REASONS: acute rheumatic fever (rheumatic endocarditis), infectious endocarditis, syphilis, diffuse connective tissue diseases, trauma, atherosclerosis.
SIGNS: There are no complaints during the compensation period.
Complaints of headache, dizziness, tendency to fainting, sensation of tremors and pain in the heart area of angina pectoris;
Examination - pallor of the skin and mucous membranes, increased pulsation of the carotid arteries ("carotid dance"), synchronization with the pulse of the carotid arteries, shaking of the head (Musse symptom), pseudocapillary pulse (Quincke symptom), narrowing of the pupil during systole, expansion - with diastole (symptom of Landolfi);
Muller's symptom is the rhythmic pulsation and expansion of the tongue and tonsils.
Palpation - spilled, resistant, rising, domed apical impulse in the VI - VII intercostal space, shifted to the left and down, sometimes, pulsation in the II intercostal space on the right;
Percussion: an increase in the boundaries of relative dullness to the left, an increase in the width of the vascular bundle in the second intercostal space;
Auscultation: I tone at the apex is weakened, II tone on the aorta is weakened with rheumatic defect, with syphilitic and atherosclerotic defect II is sonorous (sometimes with a metallic tinge). A rough diastolic murmur is heard over the aorta, which is conducted to the Botkin-Erb point and amplified in the upright position of the patient. Flint's presystolic murmur is possible at the apex (due to relative mitral stenosis). Rarely, on the femoral artery is the double tone of Traube and when pressed with a stethoscope is the double noise of Vinogradov-Durozier.
The pulse is fast, high, large, jumping, rapid (P. celer, altus, magnus, salviens, frequencies);
Blood pressure: systolic - increased, diastolic - decreased, pulse - increased.
ECG: signs of hypertrophy and overload of the left ventricle and relative coronary insufficiency;
FCG: confirms auscultation data;
X-ray: dilatation and hypertrophy of the left ventricle, aortic configuration of the heart with an emphasized waist, expansion of the aorta in both directions;
Echocardiography: a change in the valve cusps, bacterial vegetation on the valve with infectious endocarditis, dilatation of the left ventricle, hyperkinesis of its walls, vibration of the
anterior cusp of the mitral valve during the diastole.
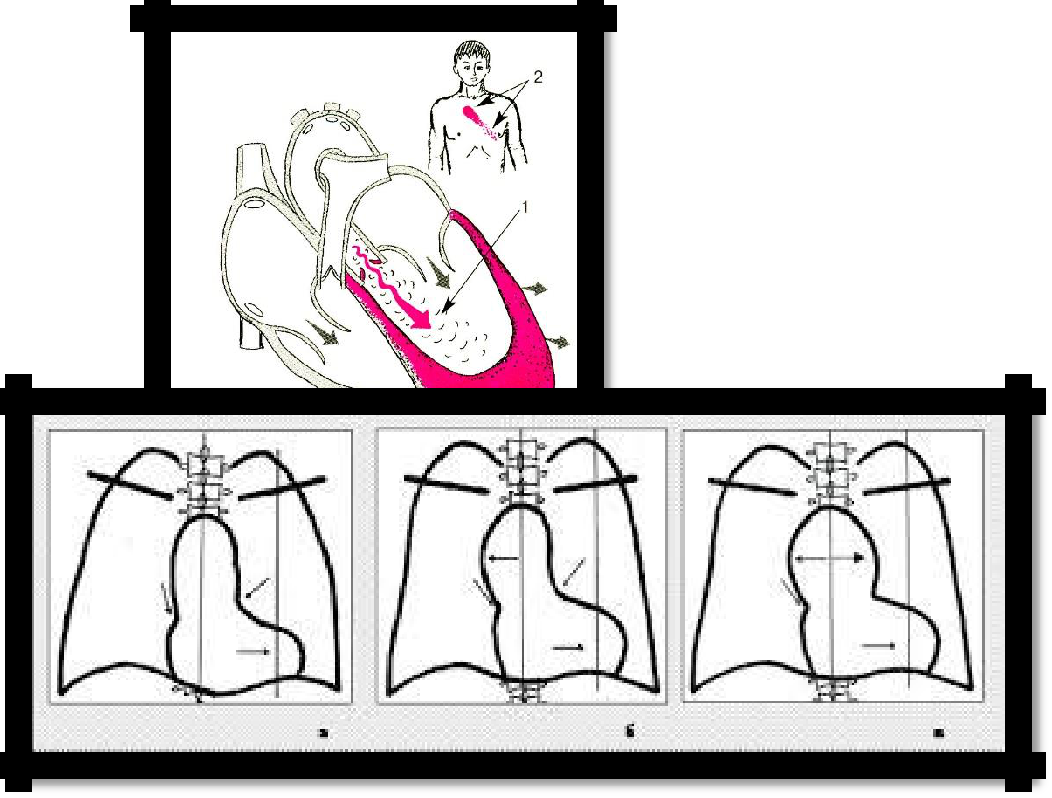
Pic 3.25 Aortic valve insufficiency (hemodynamics).
Pic 3.26 Aortic heart configuration:
Aortic stenosis (a,b); Aortic insufficiency (c)
47
14. Mitral valve prolapse
Swelling, protrusion of one or both cusps of the mitral valve into the cavity of the left atrium during ventricular systole.
CAUSES:
primary (congenital) is associated with microsomal degeneration of the fibrillar structures of the valves and / or tendon chords, often combined with defects in connective tissue structures (Marfan syndrome, flat feet, hernias, curvature of the spine, etc .;
secondary: develops against the background of heart lesions in coronary heart disease, hypertrophic cardiomyopathy, carditis of another etiology;
1. Complaints of pain in the region of the heart, especially during excitement, are not associated with physical exertion, are not removed by nitroglycerin, are inconsistent, heart failure, palpitations;
2. Auscultation: at the apex, a systolic click or late systolic murmur (or a combination of both) is determined. They increase vertically and decrease horizontally.
3. ECG: reduction or inversion of T waves, a slight decrease in the S-T segment in II, III, less often in V5 and V6 leads;
4. FCG: late systolic murmur, late systolic click;
5. Echocardiography: deflection of one, sometimes both cusps of the mitral valve in the late phase of systole into the cavity of the left atrium;
6. Doppler echocardiography: mitral regurgitation;
15. Syndrome of hypertension of the pulmonary circulation
CAUSES:
primary - 0.2% of all cases, etiology is unknown
secondary - mitral heart defects, left ventricular heart failure, some congenital heart defects with blood discharge from left to right, pulmonary thromboembolism, acute and chronic lung diseases, hypoventilation, high-altitude hypoxia, Ayers syndrome (A. Ayezza) (pulmonary sclerosis) .
SYMPTOMS:
1) shortness of breath, passing into suffocation (BH>20¢)
2) cyanosis (acrocyanosis or diffuse)
3) cough (dry or with sputum)
4) hemoptysis
5) dizziness and fainting
6) pain in the heart due to hypertrophy of the myocardium
7) angiospasm (e.g. Raynaud's syndrome)
8) possible tachycardia (heart rate > 80¢)
9) signs of right ventricular failure (see the corresponding section)
10) hypertrophy of the right ventricle (percussion, ECG, ECHO)
11) emphasis II tone over the pulmonary artery
12) wheezing (dry and wet), crepitus in the lungs
13) on the ECG - ―P‖ - high, expanded in II and III leads, hypertrophy of the right ventricle and left atrium
48
on the phonocardiogram - emphasis and splitting of II tone on the pulmonary artery
R - graph of the lungs: root compaction, thickening of the vascular pattern, cloud-like shadows, a small effusion in the pleural cavities, an increase in the right ventricle of the heart
VC is reduced
ECHOCG: increased pressure in the pulmonary artery, its dilatation, hypertrophy of the right heart.
16. The syndrome of acute vascular insufficiency
A. syncope (syncope) - a short-term, mild form of acute arterial hypotension
REASONS: acute cerebral anemia due to a mental or reflex effect on the circulatory regulation system. There are vasovagal syncope, orthostatic, sinocarotid, psychogenic, symptomatic. STAGES:
forerunners
impaired consciousness
recovery period
SYMPTOMS:
1) weakness
2) dizziness
3) ringing in the ears,
4) short-term visual impairment (veil, darkening, "flies" before the eyes)
5) pallor of the skin and mucous membranes
6) instability of the pulse, respiration and blood pressure (tachycardia, filamentous pulse, drop in blood pressure)
7) hyperhidrosis
8) decrease in muscle tone
9) short-term impaired consciousness
10) pupils dilated, slow response to light
11) patient may fall
12) short-term convulsions of a tonic, less often clonic nature
B. COLLAPSA Severe form of vascular insufficiency (a more pronounced and prolonged drop in vascular tone, leading to a violation of the vital functions of the body).
REASONS: infectious, toxic, hemorrhagic, hypoxic, orthostatic, cardiogenic, hypovolemic, sympatho-vagotonic, paralytic collapses.
SYMPTOMS:
1) consciousness is often preserved, patient indifference to the environment, lethargy, adynamia
2) dizziness
3) visual impairment, dilated pupils
4) tinnitus
5) thirst
6) chills at low body temperature
7) pointed features
8) sharp pallor with acrocyanosis
9) cold sweat
10) cold limbs
11) the pulse is frequent, small
12) venous pressure and blood pressure sharply reduced, cervical veins collapsed
13) heart sounds are deaf, arrhythmias, embryocardia are possible
14) shallow breathing (rapid or slow)
15) shock development is possible
49
Shock (from the English shock - shock, shock) is an integral pathological process that develops in response to extreme stimuli and is accompanied by a progressive violation of the vital functions of the nervous system, blood circulation, respiration, metabolism and some other functions. This is a failure of the compensatory reactions of the body in response to damage.
The clinical picture depends on the type of shock (cardiogenic, anaphylactic, infectious-toxic, post-traumatic, hypovolemic), which develops against the background of progressive vascular insufficiency.
3.1 TEST TASKS
(Choose one or more correct answers)
Pulsation of the carotid arteries ("dance carotid") is observed when
stenosis of the mouth of the aorta
aortic valve insufficiency
With increasing pressure in the pulmonary artery will be observed
attenuation of II tone on the pulmonary artery
emphasis II tone on the pulmonary artery
emphasis and II tone on the aorta
The emphasis of the II tone on the aorta is
II tone on the aorta is louder than I tone
II tone on the aorta is louder than II tone on the pulmonary artery
Indicate the most characteristic signs of arterial pulse in atrial fibrillation.
a sharp weakening or lack of pulsation on one radial artery
a sharp decrease in the pulse value on both radial arteries
the number of pulse waves in the radial artery is greater than the number of heart contractions
the number of pulse waves in the radial artery is less than the number of heart contractions
The main method for identifying endocardial syndrome
ECG
FCG
ECHO-KS
For stenosis of the mitral valve is characteristic
the rhythm of the "quail"
protodiastolic gallop rhythm
What defect is the symptom of Alfred de Musset
aortic stenosis
aortic insufficiency
mitral stenosis
mitral insufficiency
When auscultation in a patient with mitral valve insufficiency is detected
attenuation of the second tone and systolic murmur on the aorta
attenuation of the first tone and systolic murmur at the apex
clapping first tone, diastolic murmur at the apex
attenuation of the second tone and diastolic murmur on the aorta
9 Symptom characteristic of the appearance of a patient with stenosis of the aortic orifice
diffuse cyanosis of the skin
acrocyanosis
pallor of the skin
symptom of Musssi
Carotid dance
How to change the pulse pressure with stenosis of the mouth of the aorta
does not change
increases
more often decreases
3.2 Tasks for the section “Cardiovascular system”
Task 1
Patient S., 62 years old, complained of pressing pains behind the sternum and in the region of the heart that arise after psycho-emotional and physical exertion, radiating to the left arm, shoulder blade, accompanied by a sense of fear of death, stopping at rest or when taking nitroglycerin after 2 minutes.
From the medical history of the disease, it is known that an increase in blood pressure is noted over 15 years (maximum figures are 200 and 120 mmHg, adapted to 130 and 80 mmHg). For the last 2 years after psychoemotional and physical overloads, pressing pains behind the sternum occur, stopping with nitroglycerin after 2-5 minutes. From the anamnesis it is known that the patient smokes for 20 years at 18-20 cigarettes per day.
When examining a patient of increased nutrition. For centuries, xanthelasma. Percussion borders of the heart are shifted to the left. The cardiac sounds at the apex are weakened, the emphasis is II tone above the aorta. HELL 180 and 100 mmHg, heart rate-78ud. in minutes
Manifestations of what syndromes can be noted in a patient?
What are the risk factors for developing coronary heart disease in this particular case?
Task 2
Patient M., 54 years old, was taken by an emergency medical team to the intensive care unit complaining of intolerable burning pains behind the sternum, accompanied by severe weakness, cold sweat, and a feeling of lack of air. Taking nitroglycerin did not stop the pain.
Today, after physical work (lifting weights), for the first time in my life, intolerable stinging, burning pains behind the sternum appeared, radiating to the interscapular space accompanied by a sharp weakness, cold sweat. The pain was not stopped by taking 3 tablets of nitroglycerin. The total duration of the attack is 1 hour.
On examination: the patient is sitting. The skin is pale, cyanotic, covered with large drops of sweat. Bubbling breathing with the release of copious frothy pink sputum. Weakened vesicular breathing, a large number of moist, various-sized, sonic rales are heard over the lungs. Chd-26 in a minute. Heart sounds are sharply weakened, the protodiastolic gallop rhythm is heard. AD-95 and 50 mmHg Heart rate-110 per minute. The pulse on the peripheral arteries is small, filiform.
On the ECG - in leads V1-6, I and AVL, a complex of type QS, ST segment elevation of more than 5 mm (trough-shaped), negative coronary tooth T.
What syndromes can be distinguished on the basis of this clinical picture?
What disease can be thought of on the basis of this clinical picture?
Task 3
Patient V., 65 years old, came to the clinic with complaints of bursting pain in the epigastric region, accompanied by nausea, vomiting once ..