Материал: BASIC CLINICAL SYNDROMES IN INTERNAL DESEASES CLINIC
Hemolytic anemia
СAUSES.
- Congenital inferiority of red blood cells - Exposure to anti-erythrocyte antibodies - Poisoning with hemolytic poisons
Types of hemolysis: intravascular, extravascular.
SYMPTOMS. Leading syndromes: - anemic,
- hemolytic jaundice.
- Complaints: chills, fever, jaundice, nosebleeds, hematuria, hemorrhagic rash, weakness, dyspepsia, shortness of breath.
- Splenomegaly - Hepatomegaly
Blood.
Red blood cells and HB. Lowered.
Poikilocytosis, anisocytosis.
Normochromic red blood cells - normal color index (MCH).
reticulocytosis.
Positive Coombs test (intravascular hemolysis)
pro-erythronormoblasts 40-60% Urine: a lot of urobilin
Kal: a lot of stercobilin
6. Hemorrhagic syndrome
REASONS: various disorders of hemostasis and vascular permeability of hereditary or acquired origin, vasculitis.
SYMPTOMS:
bruises, bruising
petechial rash on the skin and mucous membranes
hemoptysis
bleeding from the nose, gums, stomach, intestines, urinary and genital tracts, etc.
positive tests of the tourniquet, pinch, Konchalovsky-Rumpel-Leed, etc.
The clinical manifestations of hemorrhagic diathesis are characterized by the five most common types of bleeding (Barkagan Z.S., 1975,1980):
Hematoma type
Petechial-spotted (bruise) type
Mixed (bruise-hematoma) type
Vasculitis-purple type
Angiomatous type
108

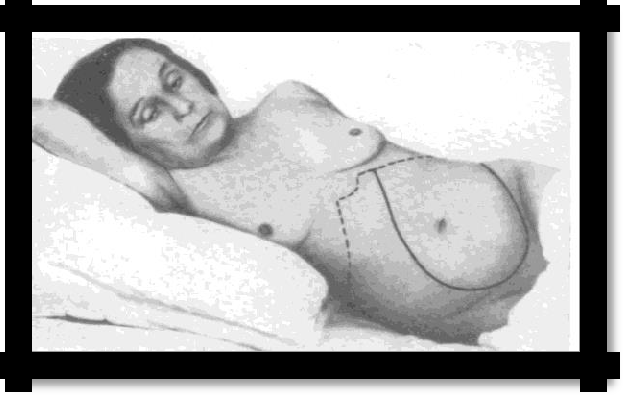
Pic 7.2 Vasculitis purple type
pic 7.3
Petechial spotted (bruise) type

(Hemorrhagic vasculitis).
7. Inflammatory syndrome
REASONS: the development of infectious complications, especially against the background of
hemoblastoses
SYMPTOMS:
fever
sore throats
abscesses
glossitis, stomatitis
picture of sepsis
any foci of infection
corresponding changes in laboratory inflammatory activity (ESR, CRP, seromucoid, etc.)
Hyperplastic syndrome CAUSES. Leukemic tissue infiltration. Symptoms
A painless enlargement of the lymph nodes, liver and spleen, tonsils (they increase significantly, become loose, can make breathing difficult).
A marked increase in the lymph nodes in the mediastinum is possible, which can lead to compression of the superior vena cava and impaired outflow of blood into the right atrium (superior vena cava syndrome with the main clinical manifestations - shortness of breath, cyanosis, swelling of the neck, swelling of the cervical veins).
Gingival hyperplasia and the development of severe ulcerative necrotic stomatitis are also characteristic, with ulcerative necrotic lesions of the tonsils, oral mucosa that extends to the pharynx and esophagus.
Ossalgia - soreness when bruising the bones due to the development of subperiosteal leukemic infiltrates.
Leukemia infiltrates appear on the skin in the form of leukemids - common reddish-bluish papule-shaped plaques.
Severe manifestations of hyperplastic syndrome are also severe painful testicular infiltration and damage to the nervous system - neuroleukemia.
Neurological syndrome
REASONS: megaloblastic, iron deficiency anemia, hemoblastosis
109
SYMPTOMS:
paresthesia, ataxia, polyneuritis
encephalopathy (strokes, paralysis, headaches)
perversions of taste (geophagy), smell (with iron deficiency anemia)
picture of funicular myelosis (with megaloblastic anemia)
10. Immunodeficiency syndrome
CAUSES. With hemoblastosis, an immunodeficiency state develops, characterized by a sharp
violation of cellular and humoral immunity, the phagocytic function of leukocytes, and a
decrease in complement activity.
SYMPTOMS
Various infectious and inflammatory processes, which, as a rule, take a severe course, often develop a septic state. Infectious and inflammatory diseases, primarily severe pneumonia, often lead to the death of patients.
However, it should be noted that fever can be a manifestation of leukemia, a transfusion reaction, spleen infarction, thrombophlebitis, which requires differential diagnosis with infectious and inflammatory diseases.
Leukemia syndrome (hemoblastosis) 11.1 Acute Leukemia Syndrome
CAUSES. Acute leukemia: myeloblastic, monoblastic, erythromyelosis, megakaryoblastic, lymphoblastic, undifferentiated, etc.
SYMPTOMS.
Leading syndromes: acute onset: often in the debut necrotic tonsillitis, stomatitis, fever. - anemic,
- hemorrhagic,
- immunodeficiency and inflammatory (septic conditions may develop), - intoxication (weakness, sweating, fever),
- hyperplastic,
- ossalgia, arthralgia,
- laboratory changes. UAC: cytopenia (leukopenia, thrombocytopenia, anemia) or leukocytosis, characterized by a leukemic failure (hiatus leucemicus) - the absence of intermediate forms between blasts and mature cells, i.e. no promyelocytes, myelocytes, metamyelocytes (young) cells. Accelerated ESR, increased CRP and LDH. A myelogram is the predominance of blast cells.
11.2 Chronic myeloproliferative syndrome
CAUSES. Chronic myeloid leukemia, true polycythemia, myelofibrosis.
SYMPTOMS (for chronic lmieloleukemia).
Leading syndromes: slow, gradual development.
anemic,
hemorrhagic,
immunodeficiency and inflammatory (septic conditions may develop),
intoxication (weakness, sweating, fever),
ossalgia, arthralgia,
hyperplastic:
splenomegaly and, less commonly, enlarged liver;
ossalgia, soreness and sensitivity when striking the bones;
110
c) a relatively rare enlargement of the lymph nodes.
laboratory changes. KLA: leukocytosis, hyperleukocytosis, all transitional forms of cellular elements: promyelocytes, myelocytes, metamyelocytes, stab and segmented neutrophils. There is no "leukemic failure." Eosinophilic-basophilic association. Accelerated ESR, increased CRP and LDH. Myelogram - single blast cells. In the blood and bone marrow is the Philadelphia chromosome.
pic. 7.4Chronic myeloproliferative syndrome
11.3 Chronic lymphoproliferative syndrome
CAUSES. Chronic lymphocytic leukemia, malignant lymphomas.
SYMPTOMS for chronic lymphocytic leukemia).
Leading syndromes: slow, gradual development, more often after the age of 40 years.
anemic,
hemorrhagic,
immunodeficiency and inflammatory (septic conditions may develop),
intoxication (weakness, sweating, fever),
ossalgia, arthralgia,
hyperplastic: a) predominant enlargement of the lymph nodes (painless, testo-elastic consistency, not soldered together, mobile);
b) the absence or moderate increase in the spleen and liver;
c) frequent skin lesions (skin infiltrates, eczema, psoriasis, herpes zoster, etc.).
laboratory changes. KLA: leukocytosis, hyperleukocytosis mainly due to mature lymphocytes, sometimes single lymphoblasts and prolymphoblasts, Botkin-Gumprecht shadow, anemia, thrombocytopenia, suppression of other sprouts. Accelerated ESR, increased CRP and LDH. Myelogram - lymphocytes (up to 90%), lymphoblasts (up to 10%), Botkin – Gumprecht shadow (up to 10-20%). Lymph node biopsy.
pic. 7.5 Lymphadenopathy
2. Disseminated intravascular coagulation syndrome
(DIC)
111
Disseminated intravascular coagulation is a complex pathological syndrome, which includes
massive blood coagulation, leading to blockage of microcirculation by loose masses of fibrin and
cell aggregates in vital organs (lungs, kidneys, liver, adrenal glands, etc.) with the development
of their dysfunction.
REASONS (etiology):
septic (especially caused by gram-negative microorganisms);
all types of shock (septic, cardiogenic, burn, hemorrhagic, etc.);
malignant neoplasms (leukemia, tumors of the lungs, stomach, etc.);
injuries (bone fractures, crash syndrome);
obstetric pathology (premature detachment of the placenta and its presentation, embolism with amniotic fluid, severe atony of the uterus, eclampsia);
acute intravascular hemolysis;
immune (immunocomplex) diseases.
hypercoagulation; II. normal coagulation; III. hypocoagulation; IV. the outcome.
SYMPTOMS: clinical manifestations are associated with ischemic (thrombotic) and hemorrhagic injuries of organs and tissues that have a well-developed microcirculatory network (lungs, kidneys, adrenal glands, gastrointestinal tract, liver, spleen, skin, mucous membranes) and are characterized by their dysfunction and bleeding of various degrees.
One of the most common, albeit optional manifestations of this syndrome is bleeding, which is observed on average in 55-T5% of patients.
Diagnosis of ICE syndrome:
1. Vascular-platelet hemostasis. Sample pinch, tourniquet, cuff test, platelet count, platelet factor determination (TF4);
2. Coagulation hemostasis: - coagulation time;
- activated partial (partial) thromboplastin time (APTT); - determination of prothrombin time;
- determination of thrombin clotting time;
- determination of fibrinogen concentration.
3. Physiological anticoagulants:
- determination of the activity of AT III (antithrombin III).
4. Fibrinolysis;
5. Methods for detecting markers of intravascular coagulation and fibrinolysis. Paracoagulation tests:
ethanol test;
-protamine sulfate test;
- determination of RFMC (soluble fibrinmonomeric complexes); - determination of PFD (fibrin degradation products).
112
7.1 TEST TASKS
(Choose one or more correct answers)
Manifestations of sideropenic syndrome are all signs, except
1) angular stomatitis
2) glossitis
3) dryness and hair loss
4) esophagitis
5) splenomegaly
Indicate the clinical manifestations of sideropenic syndrome
1) angular stomatitis
2) jaundice
3) splenomegaly
4) taste perversion
5) coilonychia
For the diagnosis of B12 - deficiency anemia, it is enough to identify
1) hyperchromic, hyporegenerative, macrocytic anemia
2) hyperchromic, hyporegenerative, macrocytic anemia and atrophic gastritis
3) hyperchromic, hyporegenerative, macrocytic anemia with the presence of Jolly bodies and Kebot rings in red blood cells
hyperchromic, hyporegenerative, macrocytic anemia and megaloblastic type of hematopoiesis
4. Petechiae are:
capillary expansion
deposition of hemosiderin in subcutaneous fat
extensive hematomas
hemorrhagic spots on the skin of a rounded shape with a diameter of 1-2 mm
hemorrhagic spots of irregular shape with a diameter of 3-4 mm
The type of bleeding characteristic of thrombocytopenia
1) hematoma;
2) petechial-spotted (microcirculatory, bruised);
3) mixed microcirculatory-hematoma (bruise-hematoma);
4) vasculitis purple;
5) angiomatous.
The diagnosis of leukemia is obvious in the presence of
1) anemia;
2) ulcerative necrotic lesions;
3) an increase in lymph nodes;
4) blastemia in the peripheral blood;
5) hemorrhages
113
Tasks for the Hematology Section
Task 1
Patient K., 56 years old, was admitted to the clinic with complaints of: general weakness, dizziness, palpitations, shortness of breath during physical exertion, tinnitus, decreased appetite, dysphagia when eating dry, solid food (Plummer-Winson syndrome). She also began to notice hair loss and increased fragility of nails. Perversions of taste appeared (desire to eat chalk, tooth powder, raw minced meat).
The above complaints appeared during the last 6 months, in the past I didn’t get sick, menopause from 54 years, menses were plentiful for 6-7 days.
On examination: the skin and visible mucous membranes are pale, seizures in the corners of the mouth, dry, flaky skin. Spoon-shaped nails, clumsy with transverse striation (koilonychia). Smoothness of the papillae of the tongue is noted. The first tone at the apex is weakened, a gentle systolic murmur is heard there, pulse - 100 beats. in min., on the jugular vein on the right is heard the "top sound", blood pressure 110 and 60 mm Hg From other organs and systems without pathology.
Clinical blood test: Red blood cells - 2.3 x 1012 / l, Hb - 38 g / l, color index. - 0.7, white blood cells - 5.0 x 109 / l, reticulocytes - 4%. ESR - 10 mm / hour. Severe red blood cell hypochromia, anisocytosis (microcytosis), poikilocytosis.
What clinical and laboratory syndromes are there in the patient?
What research is needed to clarify the diagnosis and the causes of the disease?
Task 2
Patient S., 69 years old, was admitted to the hospital with complaints of: severe weakness, fatigue, shortness of breath when walking, palpitations, dizziness, burning tongue, decreased appetite, diarrhea, pain and numbness in the lower extremities, muscle weakness ("cotton legs" ), low-grade fever.