Материал: BASIC CLINICAL SYNDROMES IN INTERNAL DESEASES CLINIC
Violation of convergence
10. Rosenbach's symptom is:
Expansion of the palpebral fissure when fixing the gaze (surprised look)
A strip of sclera when looking down between the upper eyelid and the iris
A strip of sclera when looking up between the upper eyelid and the iris
Small tremor of drooping or slightly closed eyelids
What does not apply to the clinical signs of diffuse toxic goiter:
Tachycardia
Exophthalmos
Constipation
Weight Loss
Increase in body temperature
Signs of hypothyroidism include:
Tachycardia
Exophthalmos
Constipation
Weight Loss
Increase in body temperature
What does not apply to the clinical signs of thyrotoxic crisis:
Hyperthermia up to 38-40С
Dry skin
Vomiting, diarrhea
Mental and motor anxiety
What does not apply to the characteristic complaints of patients with hypothyroidism:
Drowsiness
Chilliness
Diarrhea
Decrease in memory
Dry skin
What concerns characteristic complaints of patients with hypothyroidism:
Drowsiness
hair loss
Diarrhea
Insomnia
Weight Loss
What relates to characteristic complaints of patients with hypothyroidism:
Coarsening of the voice
Constipation
100
The increase in body temperature
Insomnia
Weight Loss
Clinical signs not characteristic of hypothyroid coma:
Arterial hypotension
Hypothermia
Diarrhea
Severe bradycardia
Oliguria, anuria
Hypoglycemic coma is characterized by all of the following, except:
The rapid development of coma
Slow development of coma
Tonic and clonic seizures
Tachycardia
Ketoacidotic coma is characterized by all of the following, except:
The rapid development of coma
Dehydration
Smell of acetone in exhaled air
The breath of Kussmaul
Autoimmune is diabetes:
1.1 types
2.2 types
3. Gestational diabetes
Insulin resistance plays a role in the development of:
Type 1 diabetes
Type 2 diabetes
Treatment of type 1 diabetes:
Diet and regular exercise
Oral hypoglycemic drugs
Insulin therapy
All of the above
Treatment of type 2 diabetes:
Diet and regular exercise
Oral hypoglycemic drugs
Insulin therapy
All of the above
In diabetes mellitus, the following plasma glucose values are detected during the oral glucose tolerance test:
Fasting ≥ 7.0 mmol / L
Fasting ≥6.1 <7 mmol / L
After 2 hours ≥11.1 mmol / L
101
4. After 2 hours ≥ 7.8 <11.1 mmol / L
In case of impaired glucose tolerance, the following plasma glucose values are detected during the oral glucose tolerance test:
Fasting ≥7.0 mmol / L
Fasting <7 mmol / L
After 2 hours ≥11.1 mmol / L
After 2 hours ≥ 7.8 <11.1 mmol / L
02
6.2 Situational tasks for the section "Endocrinology"
Task 1
Patient M., 29 years old, came to the clinic with complaints of thickening of the neck, palpitations, increased irritability, tearfulness, sleep disturbance, general sweating, trembling of the fingers, weight loss of 6 kg over the past six months, despite increased appetite. The above symptoms appeared a year ago after returning from the south. On examination: some fussiness, hasty speech pays attention. The skin is moist, hot to the touch. When examining the neck, its thickening is revealed. Symptoms of Shtelvag, Grefe - positive. Severe exophthalmos. During auscultation of the heart I, the tone at the apex is loud, there is also a gentle systolic murmur. The heart rate is 110 per min., The heart rate is incorrect: atrial fibrillation, there is no pulse deficiency.
What syndromes can be distinguished on the basis of this clinical picture?
The presence of a disease can be assumed based on available data?
Task 2
Patient L., 55 years old, was admitted to the hospital with complaints of dry mouth, thirst, skin itching, general weakness, excretes more than 2 liters of urine per day.
The above symptoms appeared 2 months ago.
On examination, it is noteworthy that the patient is of increased nutrition. The skin is dry scaly, severe rubeosis, pustular rashes.
In the study of blood tests: hemoglobin 120 mg%, red blood cells - 4.5 x 1012 / l, white blood cells - 6.0 x 109 l, ESR - 18 mm / h, glucose -12 mmol / l (240 mg%). Urinalysis: quantity - 450 ml, relative density - 1,030, protein - not available, leukocytes - 2-4 in n / a, glucose - 0.8 g / l, ketone bodies - are absent.
What disease are we talking about in this task, and what clinical symptoms are most significant for
diagnosis?
What laboratory symptoms confirm the preliminary diagnosis?
Task 3
A 25-year-old patient was delivered to the hospital ward with complaints of severe weakness, lethargy, thirst, epigastric pain, and vomiting. Deterioration after acute respiratory illness.
Objectively: inhibited, lethargic, smell of acetone from the mouth, dry skin, tongue coated with a dirty brown coating. Pulse - 100 per minute, blood pressure - 100/60 mm RT. Art. Palpation of the abdomen is painful in the epigastric region, there are no symptoms of peritoneal irritation.
Highlight syndromes
What diagnosis can be suspected?
Task 4
Patient R., 26 years old, has been suffering from diabetes since 16 years. Receives insulin therapy. After intense physical activity in the morning at 11.00 a weakness, hand tremor, sweating, restlessness, inability to concentrate appeared. The patient tried to overcome the condition by eating himself, but lost consciousness. A few minutes later came to his senses. An ambulance was called.
What condition did the patient develop?
The plan of medical measures.
Task 5
Patient., 46 years old, complains of hair loss, weakness, drowsiness, swelling of the face and limbs, coarsening of the voice, weight gain, constipation.
103
An objective examination of the face puffy, amymic. The speech is slow, "languid". The skin is dry, peeling. The thyroid gland is palpated, not enlarged. Eye symptoms are negative. Heart rate 55 per minute. HELL 100/80 mm Hg
What syndrome do you suggest?
What is the most probable reason for it?
Answers to the tasks to the section "Endocrinology"
Task 1
Thyrotoxicosis syndrome with the formation of thyrotoxic cardiomyopathy and ophthalmopathy.
Diffuse toxic goiter.
Task 2
Diabetes in favor of which they say: polydipsia, polyuria, skin itching and skin changes
Hyperglycemia, glucosuria.
Task 3
Insulin deficiency syndrome
Type 1 diabetes. Diabetic ketoacidosis
Task 4
Hypoglycemic condition
Severe hypoglycemia, characterized by impaired consciousness, requires intravenous administration of 20-100 ml of a 40% glucose solution. Alternative 1 ml glucagon solution s / c or / m
Task 5
Hypothyroidism syndrome
The most common cause of hypothyroidism is autoimmune thyroiditis.
105
7. HEMATOLOGY
1. Anemic syndrome
REASONS: anemia of any genesis, including anemia with hemoblastosis
Symptoms common to any anemia:
muscle weakness, reduced ability to work
dizziness, "flies" before the eyes
fainting
shortness of breath and palpitations when walking (decreased exercise tolerance)
pallor (alabaster with blood loss, greenish with iron deficiency (chlorosis), slightly icteric with B-12, folio-deficient anemia, with a lemon-yellow tint with hemolytic anemia) of the skin and sclera, mucous membranes.
tachycardia, systolic functional noise above the apex, pulmonary trunk. Veins: the noise of the top on vv.juqularis, etc.
a decrease in the content of red blood cells, hemoglobin, reticulocytes, the appearance of altered forms of red blood cells (micro-, macrocytes, poikilocytes, hypo-hyperchromia, etc.).
2. Sideropenic syndrome (iron deficiency)
REASONS: repeated blood loss, insufficient intake of iron with food, malabsorption, increased consumption, redistribution, hemoglobinopathies. SYMPTOMS:
complaints of difficulty swallowing dry and solid foods (sideropenic dysphagia), pain and burning of the tongue, impaired taste and appetite (the need to eat chalk, clay, coal, earth, minced meat), a perversion of smell (addiction to the smell of kerosene, acetone, etc. )
fetid rhinitis
trophic changes in the skin, mucous membranes, hair and nails: the skin is dry, slightly peeling, tans poorly, the hair is split off, it turns gray early and falls out, the nails flatten, lose their luster, have transverse striation, they break easily, spoon-like deformations of nails (koilonychia) form, ulcerations and cracks appear in the corners of the mouth, angular stomatitis, pain and burning in the tongue (glossitis)
urinary incontinence with coughing, laughing
erythrocyte hypochromia, microcytosis
decreases the level of serum iron and the total iron binding capacity of the plasma (normal 30.6
84.6 mmol / l) and increases the latent iron binding capacity (normal 16 - 44 μmol / l)
Iron deficiency anemia
CAUSES.
Inadequate intake of iron with food (strict diet, lack of fruits, meat).
Violation of iron absorption in the intestines and stomach (gastritis, enterocolitis).
Increased consumption, redistribution of iron (children, girl, pregnant, lactating women, severe inflammatory processes)).
Repeated blood loss: nasal, gastric, rectal, renal, pulmonary, uterine bleeding, in closed cavities and tissues.
Iron is not absorbed by red blood cells (hemoglobinopathies).
anemic
sideropenic.
Blood:
106
Red blood cells: less than normal. Micro, poikilo, aniso, schizocytes.
HB is below normal, a decrease in the number of reticulocytes.
Red blood cell hypochromia - color indicator (MCH) - below normal,
The content of serum iron, ferritin is reduced to less than 30 μg / l, the percentage of transferrin saturation with iron is less than 25%.
Bone marrow:
Sideroblasts <20%
B-12, folic deficiency anemia
CAUSES.
- malnutrition (lack of B-12)
- atrophic gastritis, gasterectomy
- enteritis, enterectomy (B-12, F.K. is not absorbed)
- increased consumption of B-12 and F.K. (pregnancy) - inferiority of erythroblasts (do not digest B-12, F.K.) Symptoms
Leading syndromes: - anemic;
- neurological - only with B-12 dependent anemia (gait unsteadiness, muscle weakness, pleurisy, polyneuropathy, due to the development of funicular myelosis;
- damage to the gastrointestinal tract - atrophic, inflammatory processes, resection of the stomach, small intestine, glossitis (papillae are erased, the surface is smooth, bright pink - ―varnish‖, ―raspberry‖ tongue), hepatomegaly, splenomegaly.
Blood.
- Red blood cells. Macrocytosis, megaloblasts, aniso- and poikilocytosis. - Nv. below normal, decreased reticulocyte count.
- Hyperchromia of red blood cells - raising color index (MCH). - Polysegmentation of neutrophil nuclei.
- Jolie Taurus, Kebot rings (the remains of the nucleus in red blood cells). - Indirect bilirubin over 34 μmol / L
- Raw iron> normal. The content of Vit B-12 and folic acid is reduced. Bone marrow.
- Megaloblasts.
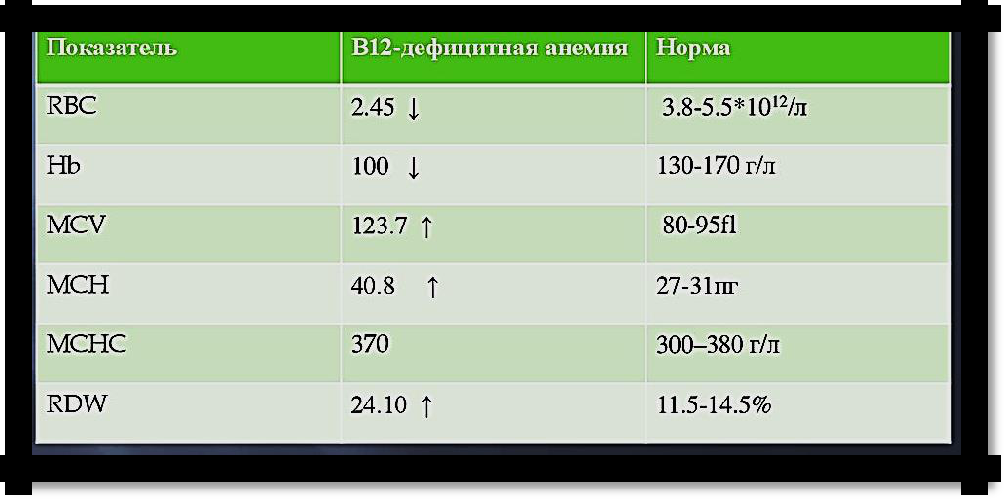
Pic 7.1 Anemia blood rates
107