Материал: BASIC CLINICAL SYNDROMES IN INTERNAL DESEASES CLINIC
6. The syndrome of accumulation of air in the pleural cavity
REASONS: occurs when bronchi communicate with the pleural cavity (subpleural location of the tuberculous cavity, abscess), with chest injury, spontaneous, artificial pneumothorax, etc. SYMPTOMS:
respiratory dyspnea;
On examination - protrusion and limitation of mobility of the corresponding side, smoothing of intercostal spaces;
If the air pressure in the pleural cavity is large, there is an increased resistance to intercostal spaces;
Voice jitter is weakened or absent;
With percussion: on the sore side - a loud tympanic tone, sometimes with a metallic tint. If the air pressure is high, the percussion tympanic tone may be blunted.
Auscultatory: breathing and bronchophony are weakened or absent (closed pneumothorax). If there is a message between the pleural cavity and the bronchus, amphoric breathing can be heard, bronchophony in this case is enhanced;
11
X-ray: a bright pulmonary field without pulmonary pattern, and closer to the root - the shadow of a compressed lung. With intense pneumothorax - displacement of the mediastinal organs to the healthy side;
With the simultaneous accumulation of liquid and air (Hydropneumothorax) in the pleural cavity, the horizontal upper limit of dullness corresponds to the level of the liquid. Dullness easily changes its boundary when changing the position of the patient's body. This border usually remains horizontal, with a loud tympanic sound above it. When succussion is determined by the noise of the splash (taking Hippocrates) in the chest.
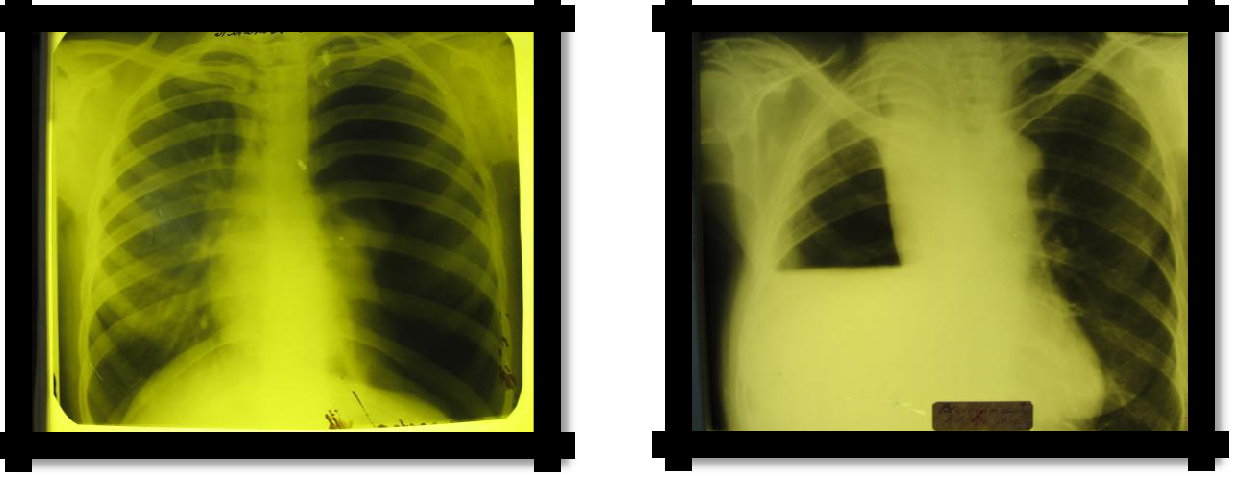
Pic 2.6 Pneumothorax Pic 2.7 Hydropneumothorax
7. Bronchiectasis Syndrome
REASONS: clinically manifests itself in the development of a chronic purulent process in altered
dilated bronchi.
SYMPTOMS:
Cough with sputum (mucopurulent, sometimes three-layer), mainly in the morning (2/3 of daily sputum: "morning toilet of the bronchi"), hemoptysis. "Dry" bronchiectasis has no clinical manifestations, with the exception of hemoptysis;
Hard breathing, dry and wet rales are possible with a compact arrangement of bronchiectasis;
X-ray: amplification, ―cellularity‖ of the pulmonary pattern (not always detected). The "gold standard" of the study is bronchography (contrasting of the bronchi with iodolipol), reveals the characteristic saccular and spherical extensions of the bronchi. Recently, computed tomography
(CT) with contrast has been widely used.
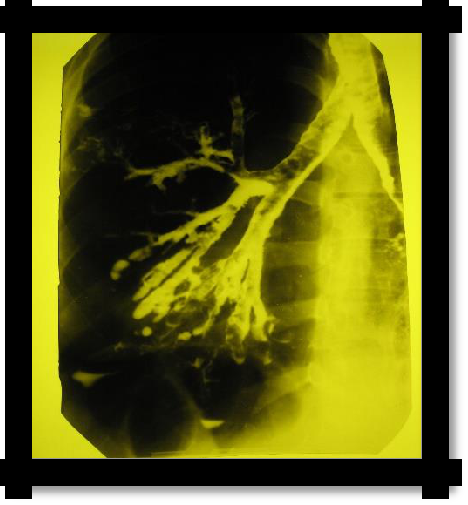
Pic 2.8 Bronchography
12
8. Syndrome of lung atelectasis
Usually distinguished: obstructive, compression and distensional (functional) atelectases
I. REASONS: obstructive atelectasis (bronchus is blocked by a tumor, thick mucus or a foreign body):
SYMPTOMS:
chest lag in the act of breathing;
voice jitter is not detected;
blunting or tympanic percussion sound;
respiration and bronchophony are not determined;
X-ray: intercostal space narrowed, homogeneous darkening in the atelectasis and mixing of the mediastinum to the affected side (Goltsknecht-Jacobson symptom), high standing of the diaphragm.
II. REASONS: compression atelectasis (the bronchus is free, the lung is squeezed by exudate, air, a large spleen through the diaphragm, etc.).
SYMPTOMS in the area of the dormant lung:
voice trembling enhanced;
blunt-tympanic percussion sound;
Weakened vesicular breathing, often with a bronchial tinge, crepitus is possible. Bronchophony is enhanced;
X-ray: increased pulmonary pattern or homogeneous darkening in the area of atelectasis.
The clinical picture of the disease that caused atelectasis (see syndromes of accumulation of air and fluid in the pleural cavity).
III. REASONS for distensible atelectasis (weakness of the respiratory movements, decreased tone of the respiratory muscles, when the pressure from the organs of the abdominal cavity, the lungs do not completely straighten and contract - tightening).
SYMPTOMS: the lower border of the lungs is 1-2 ribs above the norm, above the lower sections breathing is weakened by vesicular, crepitus and ―rattling‖ rales, which often disappear after several deep breaths.
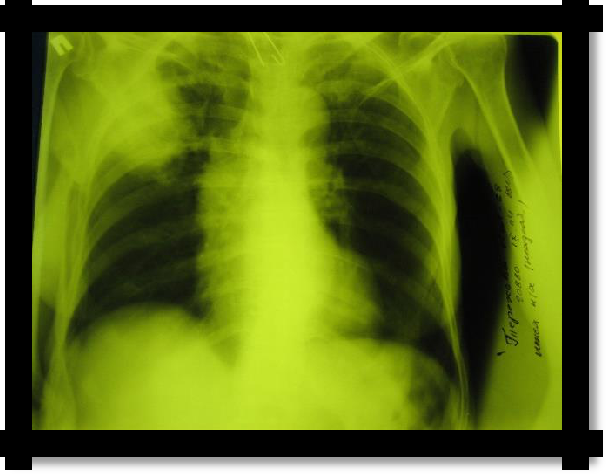
Pic 2.9 Obstructive atelectasis
13
9. Syndrome of dry pleurisy (pleuritis)
REASONS: more often a consequence of other diseases (pneumonia, tuberculosis, systemic
diseases of the connective tissue, uremia, etc.).
SYMPTOMS:
Pain in the chest, which intensifies with deep breathing and coughing;
Superficial breathing, limiting the mobility of one half of the chest. The patient lies on the affected side;
Percussion: limitation of the mobility of the lower border of the lung on the side of the lesion;
The noise of pleural friction during auscultation, sometimes confirmed by palpation;
With diaphragmatic pleurisy, pain radiates to the upper half of the abdomen or along the phrenic nerve to the neck. With apical pleurisy - pain during palpation of the trapezius muscles and pectoralis major muscles (Sternberg and Pottenger symptoms, respectively).
X-ray: on the side of the lesion, a high standing of the diaphragm, limitation of excursion of the lower edge with fluoroscopy, signs of a disease that caused pleurisy.
10. Respiratory failure syndrome
REASONS: is a complication of any severe pathological process or disease or a secondary lesion of the respiratory system.
Respiratory failure is a pathological condition of the body in which the normal gas composition of the blood is not maintained or is achieved due to the strain of compensatory-adaptive mechanisms leading to a decrease in the functional capabilities of the body. SYMPTOMS:
The most constant and leading sign of respiratory failure is shortness of breath. The severity of dyspnea reflects the degree of respiratory failure.
According to the classification of A.K. Dembo, proposed back in 1954 and currently used, 3 degrees of respiratory failure are distinguished:
degree. Latent (asymptomatic) RF (shortness of breath with moderate and significant physical exertion, the gas composition of the blood at rest is not changed).
degree. Compensated RF (shortness of breath with slight physical exertion, at rest - hypoxemia, no hypercapnia, compensatory mechanisms are already at rest).
degree. Decompensated RF (shortness of breath at rest, hypoxemia and hypercapnia).
In the diagnosis of respiratory failure, Stange tests are widely used - breath holding at the height of inspiration and Gencha - holding the breath at the height of exhalation. The lower limits of the norms of these samples are 40 and 20 s.
Another mandatory and universal sign of respiratory failure is diffuse cyanosis.
With severe respiratory failure are possible: forced body position (for example, the position of orthopnea in an attack of bronchial asthma), erythrocytosis, tachycardia, a change in the gas composition of the blood (pulse oximetry).
Change in spirometric indicators.
obstructive;
restrictive;
mixed.
Table 2.2 Classification of respiratory failure by the state of blood gases
-
degree
Р О2, мм рт.ст.
Sp02, %
Normal level
>80
>95
I
60-79
90-94
II
40-59
75-89
III
<40
<75