Материал: BASIC CLINICAL SYNDROMES IN INTERNAL DESEASES CLINIC
1. Concepts of symptoms and syndromes
During the study of the patient, one or other signs or symptoms of the disease can be identified.
Distinguish between objective and subjective symptoms:
Objective signs can be detected with the help of sensory organs (for example, changes in color, texture, shape and size of a part of the body), special equipment (ECG, radiography) or measured with special techniques.
Subjective signs are the sensations of the examined people about whom they talk (pain, nausea) or which can be guessed by their behavior, motor, clinical, vegetative-vascular reactions.
By diagnostic value, there are: pathognomonic, specific and nonspecific symptoms. Pathognomonic symptoms occur only with any one disease. For example, vomiting pus with purulent gastritis, gouty cones with gout. At the same time, diseases with pathognomonic symptoms are comparatively few, and not all patients with these diseases have pathognomonic symptoms. Therefore, an accurate diagnosis on one basis is difficult to establish.
Specific symptoms make it possible to suspect a lesion of one organ. For example, cough indicates damage to the respiratory system, jaundice - damage to the liver.
Nonspecific or general symptoms indicate that a person is sick, but does not allow a specific judgment on the nature of the disease. For example, chills, emaciation, leukocytosis. At the same time, the severity of general symptoms characterizes the severity of the disease and largely determines the prognosis.
The next step in the diagnostic process is a logical analysis of the symptoms and their grouping into syndromes.
Syndrome is a set of symptoms combined by a common pathogenesis and characterizing a certain pathological condition of the body.
The basis of the development of the syndrome can be:
Structural changes in the body - for example, valvular heart disease (these are anatomical syndromes);
Functional changes - for example, arterial hypertension syndrome (these are functional syndromes);
Some pathological conditions of the whole organism - for example, fever, syndrome of an infectious-inflammatory process (these are common syndromes);
There are also simple and complex, large syndromes. Large syndromes are a complex of pathogenetically related symptoms and syndromes. For example, the syndrome of chronic renal failure (uremia) includes more than 10 syndromes, such as anemic, polyserositis, neurological, etc. All of them are determined by one mechanism - self-poisoning of the body by nitrogenous slags that are not excreted by the affected kidneys.
Eponymous symptoms and syndromes are also distinguished (signs that got their name from the proper names of researchers, who first described them, literary or mythological characters, etc.). We presented some of them in our methodological guide.
6
2. Pulmonology
1. Syndrome of compaction of lung tissue (decrease in airiness)
REASONS: inflammatory infiltration (pneumonia, tuberculosis, non-infectious pneumonitis), pulmonary infarction, pneumosclerosis, carnification, tumors, parasitic cysts, etc. SYMPTOMS (for lung tissue infiltration):
Shortness of breath of an inspiratory character.
Unilateral reduction (restriction) of the respiratory excursion of the chest;
Strengthening of voice trembling as a result of the best conduct of oscillatory movements of the densified lung tissue;
Shortening or complete dullness of percussion sound over the sealed portion of the lung, depending on the degree of compaction;
The appearance of bronchial breathing over the background of blunting with extensive compaction: (depending on the size of the compaction, the amount of normal alveolar tissue surrounding it, options for bronchovascular, weakened vesicular and unchanged vesicular breathing are possible).
For a clear bronchial breathing, two conditions are necessary: - a sufficiently extensive surface focus of compaction;
- patency of the bronchus in the lesion.
Strengthening bronchophony;
Radiological - dimming or lowering the transparency of the lung tissue.
Acute alveolar consolidation has 2 main characteristic ultrasonic features:
Tissue-like sign (tissue sign). Normally, lung tissue during ultrasound is not visible, only the echogenic pleural line with artifacts extending from it is visualized. In pneumonia, the inflamed and edematous tissue of the lung, rich in fluid, becomes visible by ultrasound. Ultrasound examinations of the lung have a tissue-like sign. At the same time, the visualized lung tissue ultrasonographically resembles liver tissue (ultrasound ―hepatization‖ of lung tissue).
Shred sign (sign of uneven, torn border). The surface border of subpleural consolidation is the pleural line, most often represented by a flat line, while the deep (lower) border of consolidation is represented by an uneven ragged line. This ragged line (shred line) has a hyperechoic appearance, as it outlines the consolidation zone at the border with healthy aerated lung tissue.
Pic 2.1 Focal pneumonia
7
2. Syndrome of increased airiness of lung tissue (emphysema)
REASONS: It occurs in COPD, bronchial asthma; as a result of involutional changes; the outcome of many chronic lung diseases; emphysema SYMPTOMS:
Dyspnea of an expiratory character, patients exhale with closed lips, puffing out their cheeks (puff - "pink puff");
Cyanosis, puffiness of the face ("blue swelling");
The chest is barrel-shaped;
The amplitude of the respiratory excursion of the lungs is reduced. Often, auxiliary muscles are involved in the act of breathing;
The weakening of voice trembling and increased resistance of the chest are palpated;
In comparative percussion - box sound;
With topographic percussion, the expansion of the boundaries of the lungs, both up and down, restriction of respiratory excursion of the lungs;
Difficulties in determining the percussion boundaries of the heart, reducing the zone of absolute dullness of the heart.
Tachycardia (in response to hypoxia);
During auscultation, weakened vesicular, so-called "cotton" breathing is heard. The nature of breathing changes depending on the disease leading to emphysema or a concomitant process;
Radiologically determined increased transparency of the pulmonary fields, decreased diaphragm mobility, low diaphragm position, horizontal position of the ribs;
A spirographic study reveals: a decrease in lung capacity (VC) and maximum pulmonary ventilation (MLV), as well as an increase in residual volume.
3. Broncho obstructive syndrome
REASONS: bronchial asthma, COPD, allergoses, systemic diseases of connective tissue, foreign
bodies, bronchial tumors.
SYMPTOMS:
1)expiratory dyspnea (difficulty and prolonged exhalation); with severe bronchial obstruction, expiratory dyspnea reaches a degree of suffocation. Choking that occurs as an attack is called asthma. At the end of an asthma attack, viscous viscous sputum usually coughs up.
Unproductive, sometimes soundless cough;
During an attack of suffocation, the chest is as if in a state of forced inspiration, the boundaries of the lungs expand, the intercostal spaces bulge. With a sufficiently long course of the disease, emphysema develops and the chest becomes barrel-shaped (see Syndrome of increased airiness of the lungs).
With an attack of suffocation, patients occupy a forced position sitting with an emphasis on their hands. The respiratory muscles are included in the act of breathing;
The symmetric restriction of respiratory excursions of both lungs is determined;
Weakening of voice trembling;
Boxed shade of percussion sound over all pulmonary fields;
Auscultatory: weakened vesicular breathing with prolonged expiration, a large number of dry wheezing, buzzing wheezing. In extremely severe cases, respiratory sounds are not heard at all. A so-called ―silent‖ or ―dumb‖ lung develops;
An X-ray examination reveals increased transparency of the pulmonary fields;При спирографическом исследовании уменьшается форсированная жизненная емкость легких (ФЖЕЛ) и снижается индекс Вотчала-Тиффно, объем форсированного выдоха за 1-ю секунду (ОФВ1).
8
With peak flowmetry, the forced expiratory flow rate decreases (peak expiratory flow rate, PSV).
4. Lung cavity syndrome
REASONS: The formation of a cavity in the lung is usually preceded by compaction of the lung tissue. Most often, this is inflammatory infiltration (abscesses, lung gangrene, staphylococcal destruction of the lungs, pneumonia, tuberculosis), tumor decay, pulmonary infarction. SYMPTOMS:
Shortness of breath, often a productive cough, possibly hemoptysis;
Lag in the act of breathing of the affected half of the chest;
Strengthening of voice trembling and bronchophony;
Percussion: a blunt-tympanic sound is determined. With a large cavity located on the periphery, tympanic sound is observed;
Auscultatory: bronchial, and sometimes amphoric breathing, sonorous medium and large bubble rales are revealed.
It should be emphasized that all these signs are determined in the presence of a smooth-walled cavity of at least 4 cm in diameter, located close enough to the surface of the chest containing air, connecting to the bronchus and surrounded by a densified lung tissue. In the absence of these conditions, the cavity in the lung remains "dumb" and is detected only during x-ray examination.
X-ray (linear tomography, CT) signs of a cavity syndrome in the lung are limited enlightenment of a round or oval shape, usually against a background of blackout. A horizontal level of fluid in the cavity is characteristic if it communicates with the bronchus and contains exudate and air.

Pic 2.2 Linear tomography
5. The syndrome of fluid accumulation in the pleural cavity
REASONS: As a rule, a complication of another disease.
The causes of transudate are heart failure, kidney disease - nephrotic syndrome, hypo- and dysproteinemia.
The causes of exudate are inflammation of the pleura (pleurisy) of various etiologies (infectious exudate in pneumonia, abscess, tuberculosis; non-infectious exudate in malignant tumors, autoimmune diseases, uremia), wounds, trauma (hemothorax), chylous exudate (x). SYMPTOMS:
9
respiratory dyspnea;
On examination - protrusion and limitation of mobility of the corresponding side, smoothing of intercostal spaces;
Palpation - increased resistance of intercostal spaces, weakening or absence of voice trembling;
Percussion - dullness or absolute dullness over a liquid; directly above its level - a blunt-tympanic sound; the appearance of a dull sound on the healthy side due to displacement of the mediastinal organs (with large effusions); downward hepatic dullness. (Damuaso Line, Rauchfus-Grocco and Garland Triangles).
Auscultatory - the presence of fluid suggests the absence or weakening of breathing and bronchophony, and above the fluid level in the Garland triangle - a bronchial shade of breathing (on the effusion side).
X-ray homogeneous dimming is determined in the lower part of the pulmonary field with a characteristic oblique upper border for exudate and a more horizontal upper border for transudate. In the latter case, the process is often two-way. There is a shift in the mediastinal organs to a healthy side.
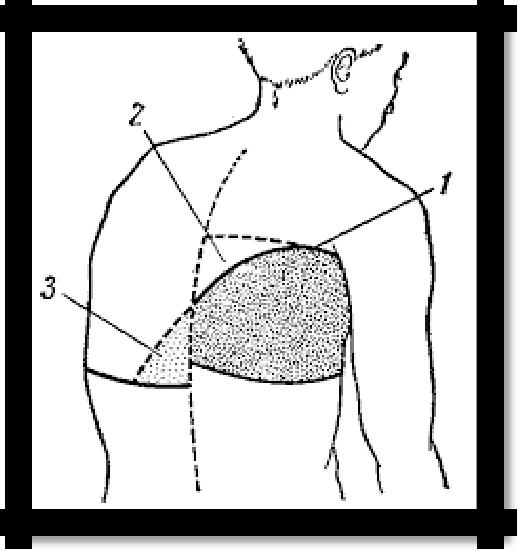
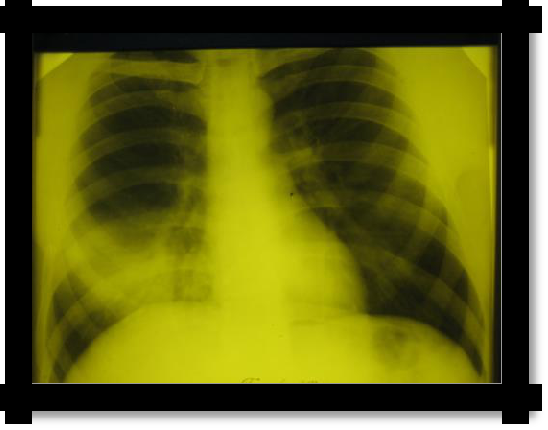
Pic 2.4 The line of Damoiso-Ellis-Sokolov (1); The Garland Triangle (2)
and the Rauchfus-Grocco Triangle (3) with exudative pleurisy.
Pic 2.5 Left-
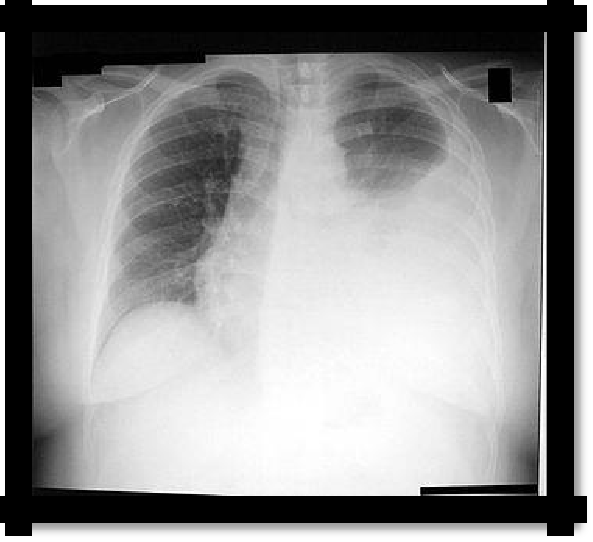
sided exudative pleuritis
10
Table 2.1 Differential diagnostic signs of exudates and transudates.
-
Type of effusion
Transudate
Exudate
Relative density
Usually
below
1.015;
rarely
Not
lower
than
1.015;
(with
compression of
large
usually 1.018
vessels by a tumor) - above
1.013-1.025
Coagulation
-
+
Color
and
Almost
transparent;
lemon
Serous
exudates
in
transparency
yellow or light yellow
appearance
do not
differ
from
transudates;
other
types
of
exudates
are
cloudy;цвет различен
Rivalt's reaction
-
+
Содержание белка
<30 g / l, usually 5-25 g / l
> 30 g / l, usually 30-50 g / l,
in purulent - up to 80 g / l
Cytological
There are few cellular elements;
There
are
more cellular
study
common
elements
than
in
mesothelial cells, red blood cells,
transudates. The number of
sometimes
lymphocytes
cellular elements,
their
predominate;
types and condition depend
after
repeated
punctures
on the etiology and phase
sometimes - eosinophils
of
the
inflammatory,
oncological processes