Материал: BASIC CLINICAL SYNDROMES IN INTERNAL DESEASES CLINIC
Answers to the tasks
Task 1
The piercing nature of the pain, as well as their relationship with breathing and coughing indicate a pleural origin of pain. The accumulation of fluid in the pleural cavity, eliminating the contact of the pleural sheets, led to the disappearance of pain.
a) respiratory failure syndrome, b) fluid accumulation syndrome in the pleural cavity,
c) intoxication syndrome
3. a) acute right-sided pneumonia complicated by exudative pleurisy, b) tuberculosis
Task 2
The appearance of harsh breathing is most likely due to inflammatory swelling of the mucous membrane of the bronchi, with a heterogeneous change in their lumen.
a) intoxication, b) damage to the mucous membrane of the bronchi, accompanied by their swelling and exudation of liquid secretion into the lumen.
The described clinical picture is characteristic of acute catarrhal bronchitis, combining (as part of an acute respiratory disease) with acute rhinitis laryngitis and tracheitis.
Task 3
a) syndrome of bronchial obstruction, b) syndrome of increased airiness of the lung tissue, c) respiratory failure syndrome
The most likely seems to be the presence of a mixed form of bronchial asthma in a patient.
With the continuation of the asthma attack over 12 hours, its transition to asthmatic status is possible.
Task 4
a) syndrome of overlay on the pleura (dry pleurisy), b) intoxication syndrome
When the patient is on a healthy side, the mobility of the pleural sheets on the "sick" side increases, which causes increased pain.
Taking into account the young age of the patient, the presence of a bend of the Mantoux test, as well as the absence of other causes of pleural damage (acute pneumonia, pulmonary infarction, connective tissue disease, malignant neoplasms, pancreatitis, etc.), the tuberculous nature of dry pleurisy should be excluded first of all
Task 5
Based on the available data, the following syndromes can be distinguished:
intoxication syndrome, b) respiratory failure syndrome, c) pulmonary tissue compaction syndrome.
The presence of crepitus is due to the appearance in the lumen of the alveoli of a small amount of exudate, leading to the adhesion of the walls of the alveoli during exhalation and their disintegration during inhalation.
Based on the available data, it can be assumed that the patient has right-sided lower-lobe (croupous) pneumonia.
Task 6
1. The following syndromes can be distinguished:
a) intoxication syndrome, b) respiratory failure syndrome, c) lung cavity syndrome
You can think about the presence in the patient of an abscess (infectious destruction) of the lower lobe of the right lung.
One should be wary of the development of pulmonary hemorrhage in the patient, empyema of the pleura, pyopneumothorax, sepsis, as well as the occurrence of new abscesses in a healthy lung.
Task 7
The following symptoms can be distinguished:
respiratory syndrome, insufficiency, b) syndrome of bronchial obstruction, c) syndrome of increased airiness of lung tissue.
With topographic lung percussion, one can expect displacement of the upper and lower boundaries of the lungs (up and down, respectively), expansion of the Krenig fields, decrease in the mobility of the lower edges of the lungs.
3. The patient has chronic, obstructive bronchitis, pulmonary emphysema.
Task 8
a) respiratory failure syndrome, b) focal pulmonary tissue densification syndrome, c) intoxication syndrome
When the focus of compaction is located in the depth of the lung tissue, the inhalation may have the features of vesicular respiration, and on the exhalation - bronchial respiration.
The patient has left-sided focal pneumonia. Its occurrence was promoted by inhalation of an anesthetic irritating to the bronchi during anesthesia, as well as the patient's stay in bed in the postoperative period.
Task 9
a) pulmonary tissue compaction syndrome, b) intoxication syndrome, c) respiratory failure syndrome
The most common hemoptysis occurs in the following diseases:
tuberculosis, b) bronchiectasis, c) abscess and gangrene of the lungs, e) malignant tumors of the lungs, e) mitral stenosis.
3. Most likely, the patient has cancer of the left upper lobar bronchus.
Task 10
a) syndrome of damage to the mucous membrane of the bronchi, b) syndrome of respiratory failure, c) nephrotic syndrome.
The patient suffers from bronchiectasis.
Against the background of a long-standing purulent infection, the patient developed amyloidosis with damage to the kidneys, liver, and spleen. To confirm this diagnosis could be the study of biopsy samples of the mucous membrane of the rectum and gums.
3. Cardiology
1. Syndromes of coronary insufficiency
By coronary insufficiency is understood circulatory disorders in the coronary vessels, in which, under physiological conditions, about 5% of all blood discharged into the aorta flows.
In clinical practice, acute and chronic coronary insufficiency are distinguished. Acute coronary insufficiency occurs suddenly or within a few minutes. An important role in its origin is played, first of all, by disturbances in the functional state of the coronary arteries (spasm, dystonia), coronary artery thrombosis, as well as rapidly occurring relative coronary insufficiency.
Chronic coronary insufficiency develops gradually, has a progressive character, it is based on a variety of long-term, recurrent and progressive lesions of the coronary artery, leading to their persistent narrowing, or occlusion.
The most common cause of acute and chronic coronary insufficiency is atherosclerosis of the coronary arteries, less commonly other diseases: rheumatism, periarteritis nodosa, systemic lupus erythematosus, infectious endocarditis.
2. Angina pectoris syndrome (stenocardia)
This is a characteristic attack of pain behind the sternum caused by transient myocardial ischemia due to insufficiency of coronary circulation.
BASIC SYMPTOMS:
paroxysmal;
characteristic localization and irradiation of pain;
short duration of the attack (no more than 20-30 minutes);
relief of pain by taking nitroglycerin or stopping the load.
Pain behind the sternum or to the left of it of a different nature: burning, squeezing, compression, heaviness that occurs during physical exertion, under the influence of cold, wind, emotional stress, at rest.
Irradiation of pain: in the left shoulder, left arm, left half of the neck or upper abdomen. Duration of pain from a few seconds to 30 minutes (usually 2-10 minutes). The pain stops when physical activity is stopped, and nitrates are taken.
On the ECG, there may be no changes outside the seizures. During an attack of angina pectoris or tests with physical activity, flattening or inversion of the T wave, depression of the S-T segment, various rhythm and conduction disturbances are possible.
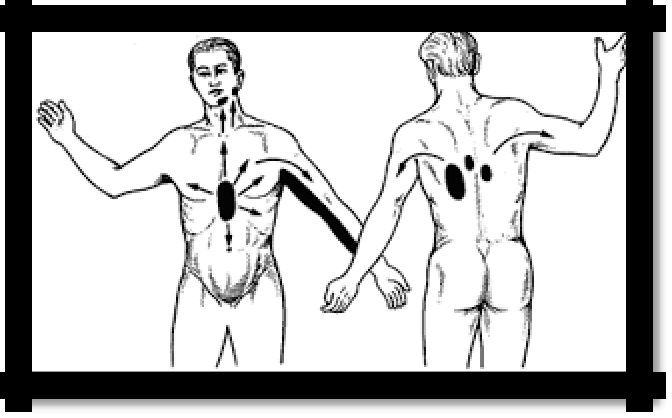
Pic 3.1 Localization and irradiation of pain in angina pectoris
26
3. Myocardial infarction is ischemic necrosis of the area of the heart muscle that occurs as a result of an acute discrepancy between the oxygen demand of the myocardium and its delivery through the coronary arteries.
Depending on the characteristics of the symptoms, 6 main clinical options are distinguished:
painful or anginal (status anginosus);
asthmatic (status astmaticus);
abdominal (status abdominalis, gastralgicus);
arrhythmic;
cerebrovascular;
asymptomatic or low-symptom.
The most common pain variant of myocardial infarction, the main manifestation is pain.
Pain with I.M. in many ways resembles angina pectoris, but differs from it in greater strength, duration and lack of effect after taking nitroglycerin, is accompanied by changes in hemodynamics (drop in blood pressure up to the development of shock, development of arrhythmias, blockade, etc.).
ECG changes are characteristic: ST segment elevation (Pardi plateau), deep Q wave, negative T wave, decreased R wave amplitude.
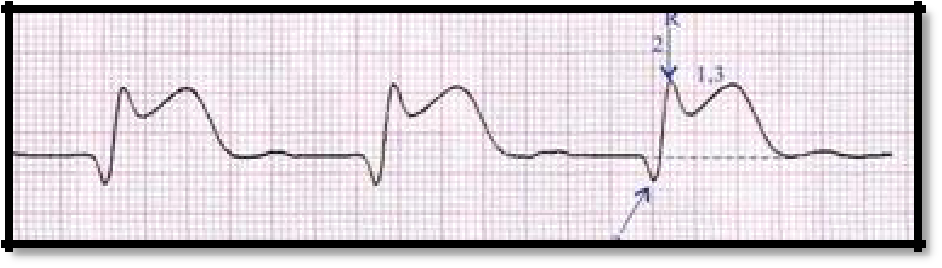
Pic 3.2 ST elevation, deep Q wave, lower R wave amplitude.

Pic 3.3 Negative T wave
4. Myocardial damage syndrome
REASONS: myocardial infarction, myocarditis, cardiomyopathy, severe heart failure, other
lesions of the mokard.
SYMPTOMS:
deafness of tones, weakening of I tone, gallop rhythm;
brady and tachycardia;
arrhythmias;
hypotension, ―headless‖ arterial hypertension (a decrease in only systolic blood pressure, and diastolic remains high).
ECG changes characteristic of causative diseases.
27
5. Resorption-necrotic syndrome
REASON: myocardial infarction
SYMPTOMS:
fever
leukocytosis, a neutrophilic shift to the left (in the first 3-5 days) and aneosinophilia, an increase in ESR (from 5-7 days), that is, a characteristic symptom of myocardial infarction ―cross‖ (a symptom of ―scissors‖) between the number of leukocytes and ESR, which is usually observed at the end of the 1st - beginning of the 2nd week of the disease: leukocytosis begins to decrease, and ESR increases;
an increase in intracellular enzymes: aspartate aminotransferase, alanine aminotransferase (AST, ALT), creatine phosphokinase (CPK), lactate dehydrogenase (LDH) myocyte structural proteins (myoglobin, troponin)
the appearance of C - reactive protein
6. Post-infarction syndrome (Dressler's syndrome).
REASON: myocardial infarction (the result of immunopathological changes). This complication usually occurs at 2-6 weeks of myocardial infarction. SYMPTOMS:
pericarditis
pleurisy (pneumonitis)
polyarthralgia up to polyarthritis (or monoarthritis)
fever
leukocytosis, eosinophilia, increased ESR
7. Аrterial hypertension Syndrome (ah)
CAUSES:
1. Primary - hypertension (essential hypertension) develops as a result of primary dysfunction (neurosis) of higher vasodilating centers in the absence of a causal relationship with organic damage to any organs or systems.
2. Secondary - symptomatic hypertension is a symptom of certain diseases or organ damage involved in the regulation of blood pressure. Symptomatic hypertension is divided into renal, endocrine, hemodynamic, neurogenic.
The nature of the increase in blood pressure distinguishes three forms of hypertension:
1. systolic;
2. diastolic;
3. systolic-diastolic.
According to WHO criteria (1999), there are three degrees of blood pressure increase, depending on systolic (SBP) and diastolic (DBP):
1st degree: increase in SBP to 140-159 mm. Hg and DBP up to 90-99 mm. Hg;
2nd degree: GARDEN - 160-179 mm Hg, DBP - 100-109 mm Hg;
3rd degree: GARDEN 180 mm Hg and above, DBP 110 mm. Hg and higher.
SUPPORT SYMPTOMS:
1. increase in blood pressure above 140/90 mm. Hg;
2. hypertrophy of the left ventricle;
3. emphasis II tone on the aorta.
SYMPTOMS:
1. headache, dizziness, fainting;
2. nausea, vomiting;
28
3. nosebleeds;
visual impairment, "flies" before the eyes;
frequent urination;
palpitations;
pain in the region of the heart (aching, stitching) and, sometimes, by the type of angina pectoris;
speech disorders, coordination of movements;
facial flushing or pallor;
throbbing of the jugular fossa, aa. carotis;
p. plenus, magnus, durus;