Материал: BASIC CLINICAL SYNDROMES IN INTERNAL DESEASES CLINIC
apical impulse is displaced to the left and down, strengthened, broadened, medium or high amplitude, resistant;
the borders of the heart are expanded to the left, the aortic configuration;
emphasis of II tone on the aorta, weakening of I tone at the apex;
Blood pressure above 140 / 90mm RT. st .;
on ECG signs of left ventricular hypertrophy
Echocardiography confirms the anatomical and hemodynamic changes associated with an increase in blood pressure;
fundus: hypertensive retinal angiopathy (narrowing of arteries, dilatation of veins).
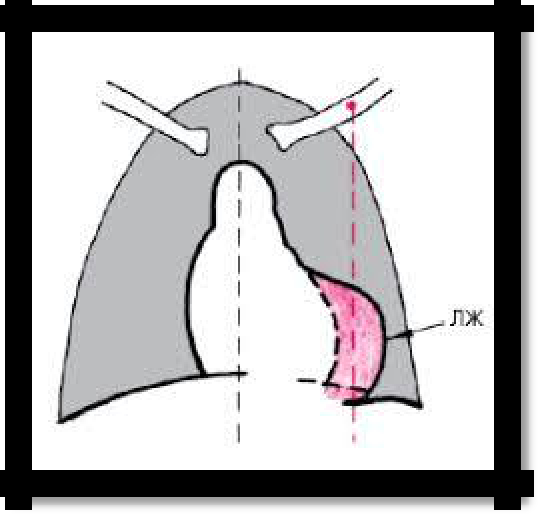
Pic 3.4 The borders of the heart are extended to the left, the aortic configuration
29
8. Arterial hypotension syndrome
Lowering blood pressure in arteries - systolic below 100 mm Hg. Art., diastolic - below 60 mm RT. Art. Distinguish between physiological and pathological arterial hypotension. A decrease in blood pressure can be observed in individuals of asthenic type, especially in an upright position (orthostatic hypotension). How a pathological symptom can be observed with shock and collapse, as a manifestation of heart or vascular insufficiency - with infectious diseases, intoxications, some lesions of the central nervous system, anemia. SYMPTOMS:
weakness, lethargy;
dizziness, fainting;
headaches, tinnitus;
visual impairment;
sometimes, cold sweat;
blood pressure below 100/60 mm Hg
pallor;
palpitations, tachycardia;
pulse of low voltage, filling.
9. Heart failure syndrome
FORMS:
acute left ventricular (left atrial);
acute right ventricular;
chronic left ventricular (left atrial);
chronic right ventricular;
total, chronic, stagnant.
CAUSES: 1) diseases that cause dystrophy, necrosis, sclerosis, inflammation and myocardial hypertrophy: heart defects, hypertension, myocarditis, thyrotoxicosis, coronary heart disease, cardiomyopathy, myocardial dystrophy, etc. 2) diseases affecting the heart from the outside: diseases of the lungs, pleura, pericardium, etc.
BASIC SYMPTOMS the severity of all manifestations depends on the severity of heart failure:
shortness of breath, often inspiratory. Sometimes as an equivalent - cough, hemoptysis;
tachycardia;
swelling, decreased urine output;
acrocyanosis, cyanosis.
With left ventricular and left atrial (with mitral stenosis) heart failure - congestion is noted in the pulmonary circulation (inspiratory dyspnea, cough, hemoptysis, moist rales, in the lower parts of the lungs, and sometimes over the entire surface of the lungs, pink foamy sputum, orthopedic. manifestations - cardiac asthma, alveolar pulmonary edema.
Right ventricular heart failure is a congestive phenomenon in a large circle of blood circulation: enlarged liver, swelling in the legs, ascites.The symptom of Kussmaul is an increase in swelling of the cervical veins on inspiration.
Positive symptom of Plesha - is characteristic of severe biventricular or right ventricular failure, is an indicator of venous stasis, high central venous pressure and volume overload. When the patient is calmly breathing for 10 s, the palm is pressed onto the enlarged liver, which causes an increase in central venous pressure by approximately 4-5 cm of water. Art. and increased swelling of the cervical veins. An abdominal-jugular test can be performed, with palm pressure being applied to the anterior abdominal wall in the umbilical region (the abdominal press should not be stressed). The result of the sample is evaluated in the same way as with the hepatic-jugular Plesha test.
30
The severity of chronic heart failure is regulated by the classification of N.D. Strazhesko -
V.Kh. Vasilenko (1935).
Stage I: initial or hidden.
It appears only during physical exertion, there are no stagnant phenomena ..
signs of fatigue (shortness of breath, sweating, finger tremors, cyanosis of the tip of the nose and lips);
slow recovery of the patient's initial state (more than 10 minutes after exercise);
with percussion of the heart, its increase is detected;
with palpation of the pulse and auscultation of the heart, tachycardia, cardiac arrhythmias, the presence of noise are determined;
increased fatigue during physical exertion.
Stage II: severe or prolonged.
Circulatory failure, not only during exercise, but also at rest.
a persistent decrease in stroke and minute blood volume;
an increase in the volume of circulating blood;
increased venous pressure, venous congestion in both circles of blood circulation, a change in water-salt metabolism;
Period IIA: stagnation mainly in the small or large circle
shortness of breath;
acrocyanosis;
transient, not very pronounced swelling of the legs and feet;
the size of the heart is increased, tachycardia is observed, sometimes arrhythmia;
a slight increase in the liver. On palpation in the right hypochondrium, the liver is painful, protrudes from under the costal margin by 2-3 cm;
single wet rales in the lower parts of the lungs;
in X-ray photographs - strengthening of the pulmonary pattern and roots of a lung of a stagnant nature.
Period IIB: congestion in both circles of blood circulation;
shortness of breath at rest (patients occupy a sitting position);
significant acrocyanosis;
massive swelling of the legs and feet;
the development of atrial fibrillation, often a tachyarrhythmic form; heart sounds are deaf, heart sizes are increased;
the liver is large, dense with a rounded or pointed edge, painful on palpation, protrudes from the costal margin by 6-10 cm;
ascites;
moist rales in the lower parts of the lungs and compaction of the roots of the lungs;
less commonly, hydrothorax and hydropericardium;
oliguria, high density of urine;
significant congestion in the organs;
severe hemodynamic disturbances;
Stage III: final or dystrophic
all the signs of period II B
exhaustion of patients (cardiac cachexia);
the skin is pale, flabby, pigmentation and trophic changes in the skin and subcutaneous tissue of the legs, significant acrocyanosis;
anasarca;
significant changes and metabolic disorders, hemodynamics;
dense edema (ascites, hydrothorax, hydropericardium);
31
an increase in heart size - cardiomegaly;
heart sounds are weakened or deaf, the heart rate is often incorrect - tachycardia, atrial fibrillation;
cardiac fibrosis of the liver (the liver is dense, enlarged, the edge is pointed, slightly painful, protrudes from the hypochondrium by 8-10 cm;
nephroangiosclerosis;
severe dysfunction of the endocrine system and c.n.s;
patients occupy a forced position (sedentary or half-sitting) due to severe shortness of breath at rest.
Table 3.1 Classification of CHF
-
CHF stages in Vasilenko-Strazhesko
Functional classes of heart failure
NewYorkHeartAssociation
(NYHA)
I st
The initial stage of the disease (heart
I fc
There are no restrictions on physical
damage). Hemodynamics is not
activity, habitual physical activity is
broken.
Latent
heart
failure
not accompanied by rapid fatigue, the
Asymptomatic LV dysfunction.
appearance of shortness of breath or
palpitations. The patient suffers an
increased load, but it can be
accompanied by shortness of breath
and / or delayed recovery of strength.
IIА
Clinically expressed stage of the
II fc
A slight restriction of physical
st
disease (heart damage). Violation of
activity: at rest, there are no
hemodynamics in one of the circles of
symptoms, habitual physical activity
blood
circulation,
expressed
is accompanied by fatigue, shortness
moderately.
Adaptive
remodeling of
of breath or palpitations.
the heart and blood vessels.
IIБ
Severe stage of the disease. Marked
III fc
A noticeable limitation of physical
st
changes in hemodynamics in both
activity: at rest, there are no
circles
of
blood
circulation.
symptoms, physical activity of lower
Disadaptive remodeling of the heart
intensity compared with the usual
and blood vessels.
loads is accompanied by the
appearance of symptoms.
III st
The final stage of heart damage.
IV fc
The inability to perform any physical
Marked changes in hemodynamics and
activity without the appearance of
severe (irreversible) changes in target
discomfort: the symptoms of HF are
organs (heart, lungs, blood vessels,
present at rest and intensify with
brain, kidneys). The final stage of
minimal physical activity.
organ remodeling.
32
Classification Comments
Stage 0 CHF in the classification is absent, because in the absence of symptoms and heart damage, heart failure in a patient is simply not. Asymptomatic LV dysfunction already corresponds to the 1st stage of the disease or, according to the severity of symptoms, to 1st FC.
To determine the stage of heart failure, as it was in the classification of V.Kh. Vasilenko and ND Strazhesko, as well as to determine FC of heart failure, as is customary in the classification of the New York Heart Association (NYHA), special procedures and studies not required.
To objectify FC CHF, an application is given with the determination of the distance of a 6-minute walk.
Determining the distance of a 6-minute walk.
This method is widely used in the last 4-5 years in international practice and allows you to assess the patient's tolerance to physical activity, using minimal technical means. Its essence is that you need to measure what distance the patient is able to go within 6 minutes. This requires only a watch with a second hand and a tape measure. The easiest way is to pre-mark the hospital corridor and ask the patient to move along it for 6 minutes. Each FC of CHF corresponds to a certain 6-minute walk:
The severity of CHF:
551 m - no heart failure
426-550 m - I FC
301-425 m - II FC
151-300 m - FC III
<150 m - IV FC
Pic 3.5 Total heart failure.
1 - significant swelling of the legs and lower back;
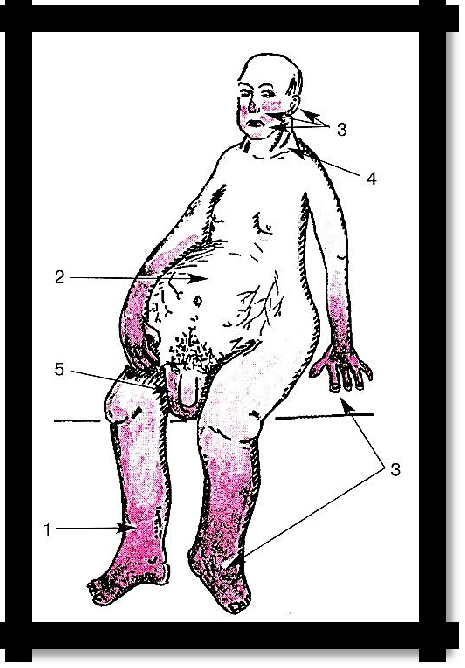
2 - ascites;
3 - severe acrocyanosis;
4 - swelling of the cervical veins;
5 - swelling of the scrotum and penis.
The patient occupies the position of orthopnea.