Материал: BASIC CLINICAL SYNDROMES IN INTERNAL DESEASES CLINIC
10. Cardiomegaly syndrome
Cardiomegaly (KMG) is a significant increase in heart size due to its hypertrophy and dilatation or accumulation of metabolic products, or the development of neoplastic processes. Causes:
1. Coronary heart disease:
a) atherosclerotic cardiosclerosis;
33
postinfarction cardiosclerosis;
aneurysm of the heart;
2. Heart defects:
acquired defects;
congenital malformations.
3. Arterial hypertension:
hypertension;
secondary hypertension.
4. Myocarditis.
5. Cardiomyopathies:
primary;
secondary.
6. The accumulation of fluid in the pericardial cavity, etc.
SYMPTOMS:
rhythm and conduction disturbance;
physical data: expansion of borders, muffling or deafness of tones, weakening of 1 tone at the apex, manifestation of the protodiastolic or presystolic rhythm of the golop (3 and 4 tones), noise of relative mitral and tricuspid insufficiency (Rivero-Carvallo noise), less often - diastolic noise of functional mitraloo stenosis (Flint) and diastolic murmur of relative pulmonary insufficiency (Graham-Steel).
Specific signs are determined by the disease that led to KMG:
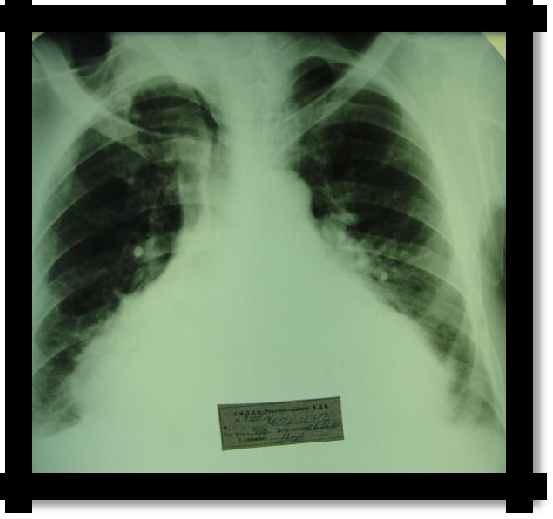
Pic 3.6 Total heart enlargement (cardiomegaly)
Syndrome of fluid accumulation in the pericardium (hydropericardium) The reasons for the accumulation of exudate:
rheumatic heart disease
tuberculosis
acute leukemia
pleuropneumonia
renal failure (uremic pericarditis)
myocardial infarction
traumatic heart damage
34
The reasons for the accumulation of transudate:
1. heart failure
Complaints: intense, persistent and increasing shortness of breath. The patient takes a sitting position with an inclination forward or knee ¾ elbow, pressing against the pillow. There are pains in the region of the heart, which intensify with breathing, coughing, body movements and are not stopped by nitroglycerin.
Examination: cyanosis, swelling of the face and neck (Stokes collar), swelling of the cervical veins, especially on inhalation due to compression of the superior vena cava by pericardial effusion, swelling on the legs, enlargement and pain of the liver, ascites. Swelling in the region of the heart and smoothness of the intercostal spaces.
With a large amount of effusion in the pericardial cavity, the patient occupies a sitting position with the body tilted forward, with his forehead resting on a pillow (Breitman symptom).
In rare cases, the patient is in the position of ―Muslim in prayer‖ (Girtz symptom - patients kneel and press their faces and shoulders to the pillow).
In some patients (especially often in men), it can be seen that the upper abdomen is not involved in breathing (Winter's symptom).
With percussion, there is a sudden transition from a clear sound over the lungs to a dull and ―hip‖ sound in the region of the heart (Auerbruger symptom).
Palpation: the apical impulse is weakened and displaced inwards from the left border of relative cardiac dullness.
Percussion: the sound above the region of the heart is dull, in some cases it has a ―wooden‖ shade. Absolute dullness of the heart usually coincides with relative dullness.
Auscultation: heart sounds are muffled or not heard, it is possible to listen to the noise of pericardial friction in the 3-4 intercostal space to the left of the sternum in the area of absolute cardiac dullness. The noise is scratching or scratching and is not carried out anywhere. He is better heard in an upright position or sitting, when the patient is tilted forward or when the head is thrown back. The pericardial friction noise is synchronized with heart contractions and usually has two amplifications - during systole and during diastole.
Radiological effusion in the pericardial cavity is characterized by a significant increase and change in the silhouette of the heart shadow. The waist of the heart is smoothed out and the shadow of the heart takes on a trapezoidal or triangular shape.
ECG: reduction of the voltage of the teeth, a change in the ST segment and the T wave in all standard leads.
12. Rhythm and conduction disturbances syndromes
REASONS: IHD (in particular, myocardial infarction, angina pectoris against the background of GB or atherosclerosis); myocarditis of various origins (rheumatic, post-influenza, infectious-allergic, toxic, etc.); heart defects (especially mitral stenosis); changes from the central and autonomic nervous system, changes in homeostasis (electrolyte imbalance, hyperthyroidism, etc.); overdose of certain drugs.
Arrhythmias: primary (atypical arrangement of the conduction pathways of the heart, the presence of additional pathways, a feature of the sensitivity of cells - pacemakers to adrenergic
35
effect); secondary (complication of the underlying disease); and on pathogenesis - organic and functional.
I. Arrhythmias due to a violation of the automatism of the sinus node:
sinus tachycardia;
sinus bradycardia;
sinus arrhythmia (respiratory).

Pic 3.7 Sinus rhythm


Pic 3.8 Sinus arrhythmia
Sinus tachycardia. Symptoms
Increased heart rate from 90 to 120 (130) in 1 minute;
Strengthening the sound of heart sounds;
On the ECG: shortening of the R-R interval, the QRS complex does not change
Sinus bradycardia. Symptoms
a rare pulse (up to 50-40 per minute);
a possible weakening of the sonority of heart sounds;
on the ECG: an increase in the R-R interval; sometimes a mild increase in the P-Q interval; atrial and ventricular complexes are not changed.
Sinus arrhythmia (respiratory). Symptoms
increased heart rate and pulse on inspiration and contraction on exhalation (this defect is eliminated when holding the breath);
on the ECG: the duration of the R-R intervals varies moderately with normal duration and shape of the teeth.
Sick sinus syndrome:
Syndrome weakness syndrome can manifest itself in the form of one of the following forms: a) latent form - there are no subjective sensations, it is clinically manifested only by bradycardia, on the ECG - a moderately pronounced sinus bradycardia;
b) manifest (hypodynamic) form - manifests itself as general weakness, dizziness, a feeling of fading in the region of the heart, passing out, speech impairment, paresis of the extremities, a rare pulse, on the ECG - sinus bradycardia, pronounced; in some patients, even attacks of Morgagni-Adams-Stokes are observed;
Short's syndrome (bradycardia-tachycardia syndrome) - is characterized by a repeated alternation of periods of severe bradycardia and tachycardia, due to the appearance of attacks of atrial fibrillation or flutter, supraventricular paroxysmal tachycardia; periodic appearance of sinoauricular blockade.
36
Arrhythmia due to disturbance of excitability:
a. extrasystole:
supraventricular (atrial and atrioventricular); ventricular (from the left or right ventricles),
polytopic (from different parts of the heart),
allorhythmia (bigeminia - every second extrasystole, trigeminia - every third, quadrigeminia - every fourth, etc.);
b. paroxysmal tachycardia (supraventricular or supraventricular and ventricular). a) Extrasystole. Symptoms
Complaints of palpitations, interruptions, sometimes, short-term ―cardiac arrest‖. Often patients do not feel extrasystoles.
9) On palpation: the pulse is arrhythmic, corresponding to the time of appearance of the extrasystole.
10) With auscultation, the premature appearance of an extrasystolic contraction of the heart, enhanced loud first tone of the extrasystole, the tones are arrhythmic.
11) If extrasystole arises quickly after the usual contraction, then with an extrasystolic contraction, the aortic valve will not open, blood will not enter the aorta and then the pulse wave on the radial artery will not be detected (pulse loss).
12) ECG is a common symptom: premature reduction in the distance R-R in front of the extrasystole is always less than that between normal contractions.
13) ECG with supraventricular extrasystoles.
Atrial extrasystole: P wave - positive, PQ shortened, QRST unchanged. If the extrasystole comes from the upper part of the atrioventricular node, then the P wave is negative; the interval is shortened; the complex has the usual supraventricular form. If extrasystole comes from the middle part of the node, then the tooth P is absent; the QRST complex does not change. If the P wave is negative from the bottom of the node and is located after the QRS complex, the P-Q interval is absent; QRS complex of the usual form. In all cases, compensatory pauses are incomplete.
T.
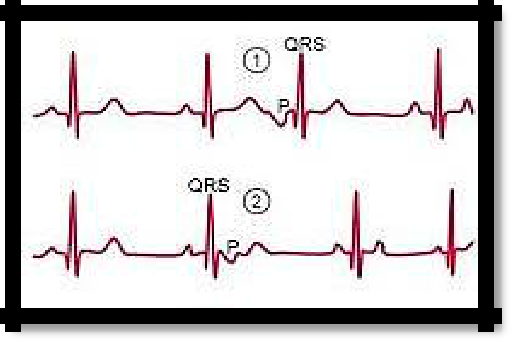
Pic 3.9 supraventricular extrasystoles(atrial and atrioventricular.
ECG for ventricular extrasystoles: P wave is absent; QRST is deformed, broadened, high amplitude; the T wave is directed back relative to the QRS; the S-T interval directly passes the tooth Complete compensatory pause.
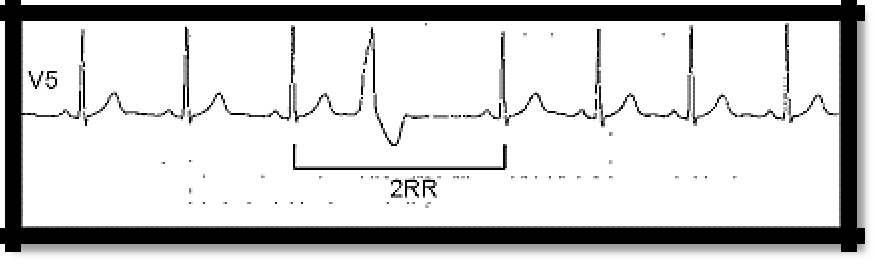
Pic 3.10 Ventricular extrasystole
37
Paroxysmal tachycardia. Symptoms
1) sudden onset of a sharp heartbeat;
2) a feeling of tightness in the chest;
3) an unpleasant sensation (sometimes pain) in the region of the heart;
4) shortness of breath;
5) general weakness;
6) nausea and vomiting;
1) pallor of the skin;
2) cyanosis with a prolonged attack;
3) swelling and pulsation of the jugular veins with an increased rhythm of up to 180-200 beats per minute;
4) rhythmic pulse (usually more than 160 per minute), small filling;
5) blood pressure may decrease;
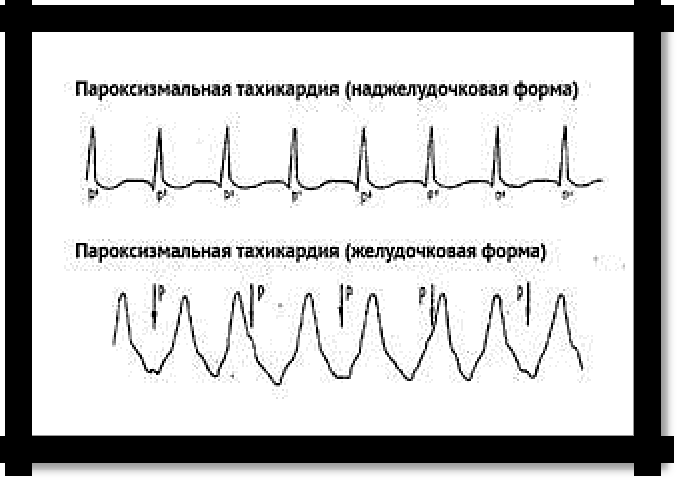
6) ECG: frequent rhythm (160 per minute and above); P wave can be registered or hidden in the QRS complex; the shape of the ventricular complex does not change (with the supraventricular form). But with the ventricular form, the QRS complex is deformed and broadened, there is no P wave.
Pic 3.11 Paroxysmal tachycardia supraventricular form and ventricular form
Flickering and fluttering: a) atrial fibrillation;
b) atrial flutter;
c) flutter and flickering (fibrillation) of the ventricles.
a) Atrial fibrillation (atrial fibrillation): tachyarrhythmic, bradyarrhythmic, normosystolic.
irregularity in the sequence of heart contractions, complete arrhythmia "delirium of the heart";
a constant change in the sonority of tones due to the different duration of diastole and different filling of the ventricles (polyphony of tones). With tachyarrhythmias at the apex, polyphony of the 1st tone is heard;
the pulse is irregular, of different filling.
heart failure
ECG:
Mandatory signs - the absence of the P wave; all R-R intervals are different;
38
7) Optional features - f waves, different in amplitude R waves.
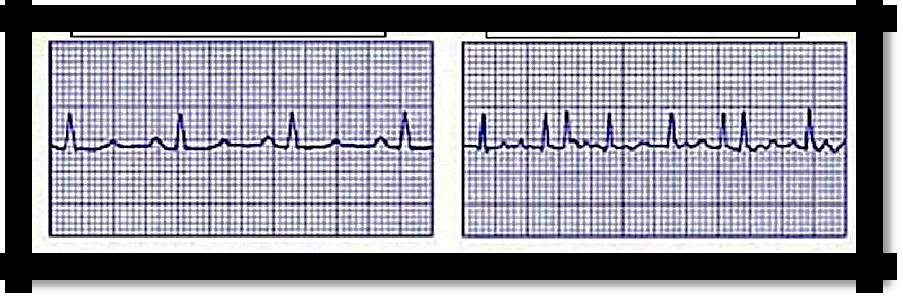
Pic 3.11 Normal ECG and Atrial fibrillation