Материал: BASIC CLINICAL SYNDROMES IN INTERNAL DESEASES CLINIC
Frequent urination, more than 6 times a day is called
oliguria
nocturia
pollakiuria
dysuria
anuria
The allocation of more than 2 liters of urine per day is called
1) oliguria
2) polyuria
3) dysuria
4) pallakiuria
5) ishuria
What sample can detect a decrease in glomerular filtration rate
1) Nechiporenko
2) Zimnitsky
3) Reberga-Tareeva
4) Addis-Kakovsky
5) Amburge
Painful urination is
pollakiuria
stranguria
ishuria
anuria
polyuria
In the formation of edematous syndrome with nephrotic syndrome, mechanisms prevail
1) violation of vascular permeability
2) system activation: aldosterone-ADH
3) decrease in plasma oncotic pressure
4) a sharp decrease in renal filtration (retention edema)
92
5) a sharp increase in hydrostatic pressure in the venous channel of blood circulation
From the symptoms below, select those that are most common for nephritic syndrome:
1) arterial hypertension
2) edematous syndrome
3) hematuria
4) hyaline and granular cylinders
5) hyperlipidemia
The main sign of nephrotic syndrome is
leukocyturia
proteinuria
hematuria
cylindruria
bacteriuria
The concept of urinary syndrome includes 1) proteinuria, edema, cylindruria
2) proteinuria, leukocyturia, hematuria
3) proteinuria, glucosuria, ketonuria
93
5.2 Situational tasks for the section "Nephrology"
Task 1
Patient M., 60 years old, was admitted to the hospital with complaints of intolerable pain in the left lumbar region with radiation to the inguinal region along the inner surface of the thigh. The patient cannot find a place for pain. Pain is accompanied by nausea, vomiting, bloating, and frequent painful urination.
Similar attacks in the patient were repeated more than once, and the patient noticed that their occurrence was associated with prolonged ―shaking" riding in vehicles.
On examination: the abdomen is soft, painless. Sharply positive symptom of Pasternatsky on the right.
Urinalysis: relative density - 1,020, yellow, cloudy, alkaline reaction, protein - absent, transitional epithelium in large quantities, leukocytes - 3-7 in the field of view, red blood cells - 15-20 in the field of view, cylinders absent, oxalates in large quantities .
What clinical syndrome can be distinguished in a patient?
What are the urinary symptoms in this case?
What disease should the patient think about?
What additional studies should be carried out by the patient?
Task 2
Patient M., 37 years old, was admitted to the clinic with complaints of common persistent edema.
For 8 years, he suffers from chronic glomerulonephritis with rare exacerbations, usually manifested by edema. The last exacerbation began 2 weeks ago: he woke up in the morning and barely opened his eyes due to edema, then the edema quickly spread throughout the body.
On examination: the face is pale, pasty, the eyelids are swollen, the eye slits are narrowed. Edema of the upper and lower extremities, lower back. Edema is soft, mobile. Heart sounds are weakened, the rhythm is correct. Pulse 88 beats per minute, blood pressure - 130 and 80 mm Hg The abdomen is soft, painless. The kidneys are not palpable. Pasternatsky’s symptom is negative on both sides. 400 ml of urine were excreted per day.
Urinalysis: amount 70 ml, relative density 1.028, transparency incomplete, protein 6 g / l, white blood cells 1-3 in the field of view, red blood cells 0-1 in the field of view, hyaline cylinders 6-8 in the field of view , granular - 2-4 in the field of view, waxy - 4-6 in the field of view, mucus and bacteria in small quantities.
What is the leading syndrome in this patient?
What research is needed to confirm this syndrome, and what symptoms can be identified in this case?
Task 3
Patient S., 27 years old, 2 weeks ago suffered a sore throat. Sore throats, fever up to 40 ° C were noted. I did not go to the doctors, I was treated myself, on the third day I went to work. Currently, edema under the eyes, more pronounced in the morning, headache, dull pain in the lumbar region, severe weakness, oliguria (excretes up to 500 ml of urine per day) is disturbing.
On examination: pallor and puffiness of the face, swelling of the lower extremities. During auscultation of the heart, I tone at the apex weakened the accent of II tone above the aorta, the
94
heart rate was correct. Pulse - 50 beats per minute, intense. HELL - 170 and 100 mm Hg 450 ml of urine were released per day.
Urinalysis: amount of 65 ml, relative density - 1,025, color - type of "meat slops", protein - 2.5 g
l, tubule epithelium cells - 1-2 in the field of view, red blood cells - 5-70 in the field of view, white blood cells - 1-3 in the field of view, hyaline cylinders - 3-5 in the field of view, granular - 2-4 in the field of view, a lot of mucus, bacteria - a small amount.
What are the urinary symptoms of this patient?
What clinical syndromes can be distinguished in this case?
What large clinical syndrome can be formulated on the basis of the data obtained?
Answers to the tasks to the section "Nephrology"
Task 1
Renal colic syndrome
Leukocyturia, microhematuria, oxalaturia.
Urolithiasis
Ultrasound examination of the abdominal organs, survey radiography of the kidneys, intravenous urography.
Task 2
Nephrotic syndrome.
Determine the daily proteinuria, the level of total protein (hypoproteinemia) and albumin (hypoalbuminemia) in the blood serum, as well as to detect hyperlipidemia, the content of cholesterol and triglycerides in the blood.
Task 3
Microhematuria, proteinuria, cylindruria.
Edema, hypertension, oliguria, urinary syndrome.
Acute nephritic syndrome.
95
6. Endocrinology
1. Syndrome of hypothyroidism:
REASONS: The disease is caused by a decrease or complete loss of thyroid function. Severe
hypothyroidism is called myxedema. There are primary hypothyroidism caused by direct damage
to the thyroid gland and secondary, developing as a result of insufficient production of
thyrotropin or thyroliberin. The most common causes of hypothyroidism are autoimmune
thyroiditis (autoimmune destruction of the thyroid gland) and thyroidectomy (postoperative
hypothyroidism). Iodine deficiency in our country exists in most regions, but it is never the cause
of hypothyroidism.
SYMPTOMS:
Damage to the nervous system: lethargy, drowsiness, lethargy, memory loss, speech slowdown, adynamia.
Cardiovascular system: bradycardia, dull heart sounds, decreased voltage of ECG teeth, decreased blood pressure, sometimes increased blood pressure (mainly diastolic), myocardial damage (myocardial dystrophy).
Damage to the skin and mucous membranes: the skin is dry, cold, dense (not folded), peeling off; hyperkeratosis of the palms, brittle nails, hair loss. The face is swimming, mask-like, the eye slits are narrow. Swelling of the lips, eyelids, cheeks, neck. When pressed on the edematous tissue, there is no fossa. Speech becomes slow, voice is low (due to the thickening of the vocal cords). The tongue is edematous. Violation of the gastrointestinal tract, constipation, belching, etc.
Edema in serous cavities (usually hydropericardium, hydrothorax) Hertog’s symptom is hair loss on the eyebrows, especially on the lateral side.
Laboratory data: hypercholesterolemia, normochromic anemia, decreased basal metabolism,
hypoglycemia, decreased levels of thyroid hormones (T3 and T4). With primary hypothyroidism, TSH increases (negative feedback principle), with secondary TSH decreases.
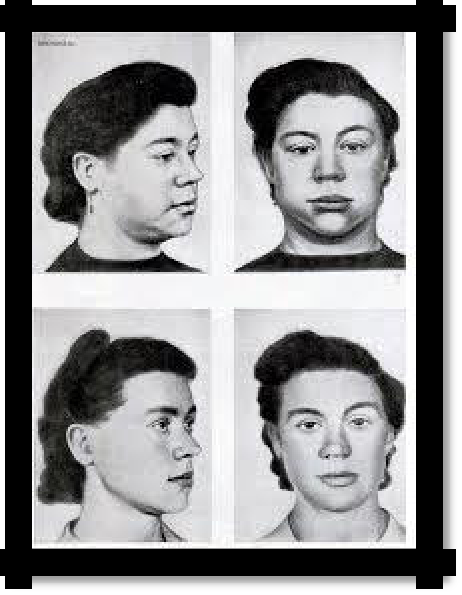
Pic 6.1 Hypothyroidism, before and after treatment.
Thyrotoxicosis syndrome (hyperthyroidism):
Thyrotoxicosis is an increase in the level of T3 and T4 in the blood and their toxic effect on the body. The term hyperthyroidism is often used as a synonym for thyrotoxicosis. However, it should be remembered that thyrotoxicosis (i.e., an excess of thyroid hormones) is not always associated with an increase in the functional activity of the thyroid gland.
96
REASONS for thyrotoxicosis: 1. Thyrotoxicosis associated with increase in the functional activity of the thyroid gland occurs with diffuse toxic goiter (Graves-Bazedov disease) or nodular toxic goiter;
Thyrotoxicosis, not associated with increase in the functional activity of the thyroid gland occurs with destruction of the thyroid gland. The destruction of the thyroid gland leads to the release of accumulated hormones (destructive thyrotoxicosis). At the same time, the functional activity of the gland is not increased. This is observed with thyroiditis (subacute thyroiditis, autoimmune thyroiditis); destructive thyrotoxicosis is always short-term and is not treated with thyreostatics. Also, thyrotoxicosis without hyperthyroidism is observed with an overdose of L-thyroxine (in this case, on the contrary, there is hypothyroidism that is treated with L-thyroxine).
SYMPTOMS:
Damage to the nervous system: nervousness, irritability, fussiness, tearfulness, sleep disturbance, memory loss, tremor of fingers and the whole body.
Symptom Marie - a small symmetrical tremor of the fingers of extended arms, as well as a "symptom of a telegraph pole" - a pronounced trembling of the patient, which is felt by the doctor upon palpation of the patient's chest.
Eye symptoms:
Gref's symptom: when the vision fixes an object that slowly falls down, a section of the sclera is exposed between the upper eyelid and the edge of the iris.
Kocher's symptom is the same when moving an item from bottom to top.
The symptom of Dalrymple is the same when fixing the object with vision in a horizontal plane, another interpretation of this symptom is wide open eye slits Rosenbach's symptom is tremor of the eyelids with closed eyes.
Symptom of Geoffrey - inability to form folds on the forehead, when looking up; Shtelvag symptom - a rare blink.
The symptom of Moebius is the eyeball moving outward when the gaze fixes an object brought to the nose bridge; indicates weak convergence due to changes in t. rectos internus.
The symptom of Stasinsky or the "red cross" - manifests itself in the form of an injection of vascular sclera. The departure of the injected vessels up, down, to the right, to the left of the iris gives the impression of a red cross in the center of which the pupil is located. Symptom Elineka - pigmentation of the eyelids.
Symptom Kraus - increased eye gloss.
Lagophthalmus - the inability to close your eyes for centuries, which in severe cases causes
ulceration of the cornea and sclera with subsequent infection.
Cardiovascular system: tachycardia, cardiac arrhythmias (extrasystole, atrial fibrillation), systolic hypertension, development of heart failure.
Gastrointestinal tract lesion: increased appetite, increased motility and gastric secretion, diarrhea, weight loss, toxic hepatitis.
Catabolic disorders: symptoms associated with increased metabolism: fever, sweating, feeling hot.
The defeat of other endocrine glands (hypogonadism, adrenal insufficiency, impaired carbohydrate metabolism).
Laboratory data: hypocholesterolemia, increase in basal metabolic rate. T3 and T4 increase, TSH decreases according to the principle of negative feedback.
97
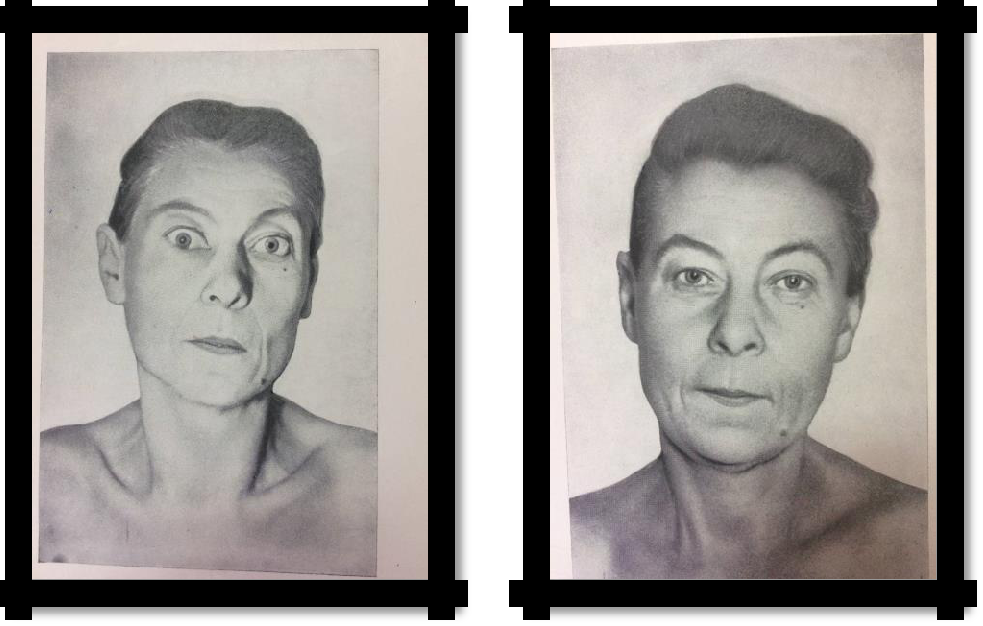
Pic 6.2 Thyrotoxicosis, before and after treatment.
3. The syndrome of insulin deficiency:
REASONS: absolute for type 1 diabetes (insufficiency of insulin secretion, a decrease in blood insulin due to the death of 100% beta cells) or relative for type 2 diabetes (defects in the receptor apparatus of insulin-dependent tissues - insulin resistance, normal or high insulin levels in the blood) , violation of insulin secretion by beta cells of the pancreas.
SYMPTOMS: "Large" - polydipsia, polyphagy, polyuria, weight loss, hyperglycemia, glucosuria, ketoacidosis. Weight loss and ketoacidosis are observed with absolute and pronounced relative insulin deficiency. Overweight and polyphagy are characteristic of insulin resistance.
"Small" - weakness, skin itching, especially in the perineum and genital area, furunculosis, tendency to infectious diseases, frequent lesions of the oral mucosa, periodontal disease, visual impairment, gastrointestinal function, large fetus, decreased body temperature.
Typical complications of diabetes.
Systemic damage to the whole organism in connection with a violation of carbohydrate and other types of metabolism and develops against their background:
poleneuropathy
macroangiopathies
microangiopathies
Diabetic coma.
Ketoacidotic
Hyperosmolar
Lactic acid (lactocidemic)
Hypoglycemic
98
6.1. TEST TASKS
(Choose one or more correct answers)
What is not typical for thyrotoxicosis?
1) exophthalmos;
2) bradycardia;
3) fussiness;
4) hand tremor;
5) sweating.
What symptom is not characteristic of hypothyroidism?
1) weight loss;
2) dry skin;
3) slowing down speech;
4) hair loss.
What is not typical for type 1 diabetes?
development at a young age;
development in old age;
development in childhood.
What is typical for type 2 diabetes?
1) development at a young age;
2) development in old age;
3) development in childhood.
For what disease is bronze color of the skin characteristic?
1) diabetes mellitus;
2) addison's disease;
3) hypothyroidism;
4) acromegaly.
The symptom of Dalrymple is:
Expansion of the palpebral fissure when fixing the gaze (surprised look)
A strip of sclera when looking down between the upper eyelid and the iris
A strip of sclera when looking up between the upper eyelid and the iris
Small tremor of drooping or slightly closed eyelids
7. The symptom of Gref is:
Expansion of the palpebral fissure when fixing the gaze (surprised look)
A strip of sclera when looking down between the upper eyelid and the iris
A strip of sclera when looking up between the upper eyelid and the iris
Small tremor of drooping or slightly closed eyelids
8. The symptom of Kocher is:
Expansion of the palpebral fissure when fixing the gaze (surprised look)
A strip of sclera when looking up between the lower eyelid and the iris
A strip of sclera when looking up between the upper eyelid and the iris
Small tremor of drooping or slightly closed eyelids
99
9. Symptom of Moebius:
Expansion of the palpebral fissure when fixing the gaze (surprised look)
A strip of sclera when looking down between the upper eyelid and the iris
A strip of sclera when looking up between the upper eyelid and the iris