Материал: MasterPass _ Pharmacology in 7 Days for Medical Students
PHARMACOLOGY IN 7 DAYS FOR MEDICAL STUDENTS
Vasodilatation and platelet |
|
aggregation inhibition |
|
Vasoconstriction & stimulation |
of platelet aggregation |
|
|
|
|
|
|
|
|
Fever, flushing (vasodilatation), |
pain & diuresis |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Prostacyclin |
|
(PGI |
|
2 |
(TxA |
|
|
|
|
|
|
|
|
PGE |
|
|
|
|
|
|
||
|
|
ThromboxaneA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
) |
|
|
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
2 |
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
||
|
|
|
|
synthase |
|
|
|
|
|
isomerase |
|
macrophages) |
|
|
|
|
|
|
||||
|
|
|
endothelial |
|
|
|
|
|
|
& |
|
|
|
|
& |
|
||||||
|
|
|
cells) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
uterus) |
|
|
synthase |
|
|
|
platelets) |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
2 |
|
|
|
|
α |
|
|
|
|
|||||
|
|
|
|
|
Thromboxane |
PGE |
|
mast |
cells |
PGF |
2 |
lungs |
|
|
||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
(in |
|
(in |
|
|
|
|
|
|
|
|
||||||||
|
|
|
Prostacyclin |
|
|
|
|
|
|
|
|
|
|
|
(in |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(in |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PGH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PGG |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COX-1 & COX-2 |
|
|
|
|
|
|
|
NSAIDs & |
COX-2 inhibitors |
|
|
|||
|
|
|
|
|
|
|
|
|
enzymes |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Arachidonic acid |
|
|
|
|
|
|
|
|
|
|
|
|
||
Bronchoconstriction & abortion |
metabolism) |
|
|
|
acid |
|
|
|
|
|
arachidonic |
PGF |
||
α |
|
|
2 |
|
|
|
|
(cyclo-oxygenase pathway of |
|
|
Figure 3.18 Prostaglandins synthesis and functions |
84
MECHANISMS OF ACTION
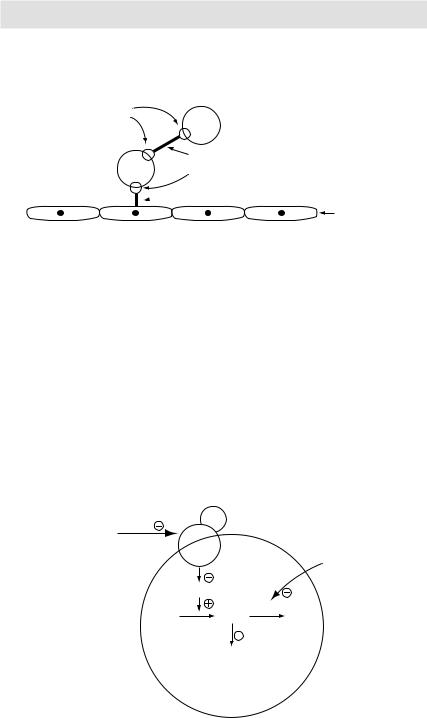
Platelets bind to vascular subendothelial collagen cells via von
Willebrand factor. Platelets bind with each other via fibrinogen strands
GPIIb-IIIa |
|
|
receptors on platelet |
Platelet |
|
membranes |
||
|
|
Fibrinogen |
Platelet |
GPIb receptors on platelet membrane |
|
 von Willebrand factor
von Willebrand factor
Subendothelial collagen cells
Figure 3.19 Mechanism of platelets adhesion and aggregation
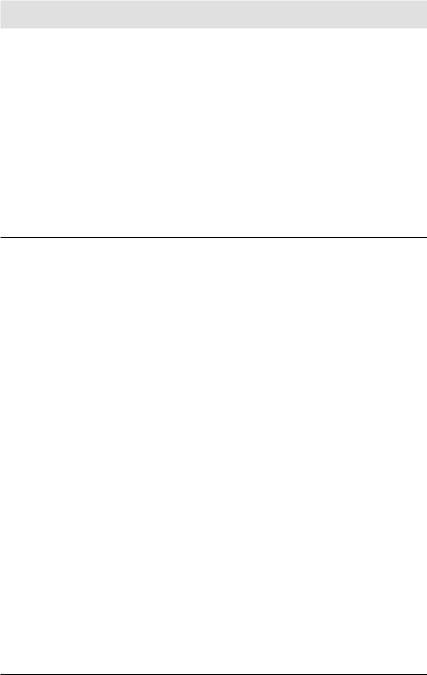
receptors present on platelet cell membranes in turn causing activation of adenylyl cyclase → ↑ intracellular cAMP → platelet aggregation inhibition. cAMP is degraded by phosphodiesterase (PDE) enzyme into inactive AMP. Dipyridamole, another antiplatelet drug, inhibits PDE → ↑ intracellular cAMP → platelet aggregation inhibition.
Methotrexate
As a DMARD: It is a disease-modifying antirheumatic drug (DMARD). It acts by inhibiting lymphoid proliferation and thus reducing the number of immune cells available to participate in the inflammatory response.
Clopidogrel |
ADP |
|
ADP |
|
|
Ticlopidine |
|
|
|
receptor |
Dipyridamole |
Adenylyl cyclase |
|
|
ATP |
cAMP PDE |
AMP |
|
|
(inactive) |
Platelet aggregation inhibition by a poorly understood mechanism
P
l
a
t
elet
Figure 3.20 ADP-dependent pathway of platelet activation
85

PHARMACOLOGY IN 7 DAYS FOR MEDICAL STUDENTS
As an anticancer drug: DNA synthetic pathway:
Methotrexate is a substrate for and inhibitor of dihydrofolate reductase. Inhibition of this enzyme blocks DNA synthesis at two points:
1It decreases the synthesis of purine and pyrimidine nucleotides.
2It decreases the synthesis of DNA from deoxynucleotides.
Cyclophosphamide
It is a prodrug that is transformed by hepatic cytochrome P450 enzymes to an alkylating agent. Just like other alkylating agents, cyclophosphamide is a cell cyclenonspecific (CCNS) drug. It damages DNA by alkylating nucleophilic groups on DNA bases (particularly the N-7 position of guanine). This leads to crosslinking of bases, abnormal base pairing and ultimate breakage of DNA strands. Cyclophosphamide is cytotoxic to proliferating lymphoid cells – both B and T lymphocytes (→ immunosuppression), although, effect on the former cells is greater.
Vincristine and vinblastine
Vinca alkaloids (vincristine and vinblastine) are cell cycle-specific agents that primarily act in the M phase of cancer cell cycle. They prevent the assembly of tubulin dimmers into microtubules. This in turn blocks the formation of mitotic spindles.
Doxorubicin and daunorubicin
These anthracyclines are cell cycle-nonspecific (CCNS) drugs. They intercalate between base pairs, inhibit topoisomerase II and generate free radicals. Free radicals in turn block the synthesis of RNA and DNA and cause scission of DNA strands.
Amphotericin B
It is a polyene antifungal agent. Polyene molecules are amphipathic, i.e. they are both hydrophilic and lipophilic. They bind to ergosterol (a sterol specifically found in the cell membranes of fungi) in turn causing the formation of artificial pores in fungal cell membranes. These pores allow leakage of intracellular ions and macromolecules eventually leading to cell death.
Nystatin
Just like amphotericin B, Nystatin is a polyene antifungal agent. Its mechanism of action is similar to that of amphotericin B.
Griseofulvin
It is taken up by sensitive dermatophytes by an energy-dependent mechanism. Once inside the cytoplasm, Griseofulvin interferes with microtubular function and inhibits synthesis and polymerisation of nucleic acids. The net result is death of dermatophytes.
Acyclovir
Acyclovir is a guanosine analogue. It is activated by a viral enzyme called thymidine kinase to form acyclovir triphosphate. The latter is incorporated into viral DNA, where it causes chain termination by inhibiting viral DNA polymerase.
Since phosphorylation of acyclovir is necessary for its antiviral effect, viral strains
86
MECHANISMS OF ACTION
that lack thymidine kinase are resistant to acyclovir. Also, a change in viral DNA polymerase so that it is no longer inhibited by acyclovir triphosphate can cause viral resistance to acyclovir.
Metoclopramide
In the enteric nervous system (ENS), metoclopramide increases upper GI motility by:
1Acting as an acetylcholine facilitator.
2Acting as dopamine receptor antagonists.
The net effect is an increase in upper GI motility with resultant alleviation of vomiting.
Antiarrhythmic drugs
Table 3.3
Class Example |
Mnemonic: MBA college Mechanism |
Ia |
Disopyramide |
Membrane stabilisers |
|
|
(Na+ channel blockage → |
|
|
membrane stabilisation) |
Ib |
Lidocaine |
Membrane stabilisers |
|
|
(Na+ channel blockage → |
|
|
membrane stabilisation) |
Ic |
Flecainide |
Membrane stabilisers |
|
|
(Na+ channel blockage → |
|
|
membrane stabilisation) |
II |
Propranolol |
Beta blockers |
III |
Amiodarone, |
Action potential widening |
|
sotalol |
agents (K+ channel blockage |
|
|
→ widening of AP) |
Na+ channel blockers (prolong the AP; intermediate dissociation)
Na+ channel blockers (shorten the AP; fast dissociation)
Na+ channel blockers (no effect on AP duration; slow dissociation)
β-Adrenoceptor blockers
K+ channel blockers
IV |
Verapamil |
Calcium channel blockers |
Ca++ channel blockers |
||
|
|
|
|
|
|
Class |
Example |
PR interval |
QRS duration |
QT interval |
|
|
|
|
|
|
|
Ia |
Disopyramide |
↓ or ↑* |
↑↑ |
|
↑↑ |
Ib |
Lidocaine |
Ð |
Ð |
|
Ð |
Ic |
Flecainide |
↑ (slightly) |
↑↑ |
|
Ð |
II |
Propranolol |
↑↑ |
Ð |
|
Ð |
III |
Amiodarone, |
↑ |
↑↑ |
|
↑↑↑↑ |
|
sotalol |
↑ |
Ð |
|
↑↑↑ |
IV |
Verapamil |
↑↑ |
Ð |
|
Ð |
Misc |
Adenosine |
↑ |
Ð |
|
Ð |
*PR interval may ↓ d/t antimuscarinic action; it may ↑ d/t Na+ channel blocking action
87
PHARMACOLOGY IN 7 DAYS FOR MEDICAL STUDENTS
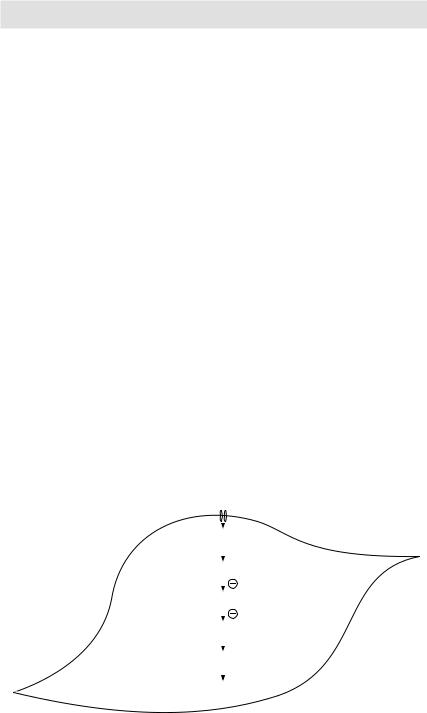
Calcium channel blockers
These drugs block voltage-gated ‘L-type’ Ca++ channels found in cardiac and other smooth muscle tissues → ↓ Ca++ influx → ↓ cytoplasmic Ca++ concentration → ↓ muscle contractility (vasodilatation, and to a lesser extent dilatation of bronchial, gut and uterine smooth muscles). All Ca++ channels blockers reduce BP. Effect on heart rate is, however, variable. Diltiazem and verapamil block Ca++-dependent AV nodal conduction → slowing of heart rate. Nifedipine and other dihydropyridines Ca++ channel blockers primarily affect the peripheral blood vessels → peripheral vasodilatation → ↓ BP → reflex tachycardia.
Note: Since ‘L-type’ Ca++ channels are not found at NM junctions and in endocrine tissues, Ca++ channel blockers do not affect the release of neurotransmitters or hormones.
K+ channel openers (minoxidil, nicorandil)
K+ channel openers (minoxidil, nicorandil), as the name suggest, open K+ channels present in the cell membranes of myocytes causing K+ efflux. The resultant hyperpolarisation makes membrane depolarisation difficult to achieve by normal excitatory stimuli. In the absence of depolarisation, voltage gated Ca++ channels responsible for Ca++ influx do not open. The resultant fall in intracellular Ca++ leads to arterial smooth muscle relaxation.
Angiotensin-converting enzyme inhibitors (ACEIs)
Physiologic role of angiotensin-converting enzyme (ACE): ACE (also known as kininase-II and peptidyl dipeptidase) is responsible for the conversion of:
1Angiotensin-I to angiotensin-II. The latter has three important effects: a It is a potent vasoconstrictor (→ ↑ peripheral vascular resistance).
b It acts on angiotensin AT1 receptors on the adrenal cortex and causes the release of aldosterone, which in turn causes Na+ and water reabsorption in exchange of K+ and H+ from the distal convoluting tubules of the nephron.
|
Ca++ |
|
|
|
|
|
Ca++ |
|
|
|
|
|
Ca++-Calmodulin complex |
|
|
|
|
|
Myosin light chain kinase enzyme |
|
|
|
|
|
|
|
|
Myosin phosphorylation |
|
|
|
|
|
|
|
|
Actin-Myosin crossbridges |
|
|
|
|
|
|
|
Myocyte |
Contraction |
|
|
|
|
Figure 3.21 Mechanism of vascular smooth muscle contraction
88