Материал: MasterPass _ Pharmacology in 7 Days for Medical Students
MECHANISMS OF ACTION
Ca++ channel  Ca++ blockers
Ca++ blockers 

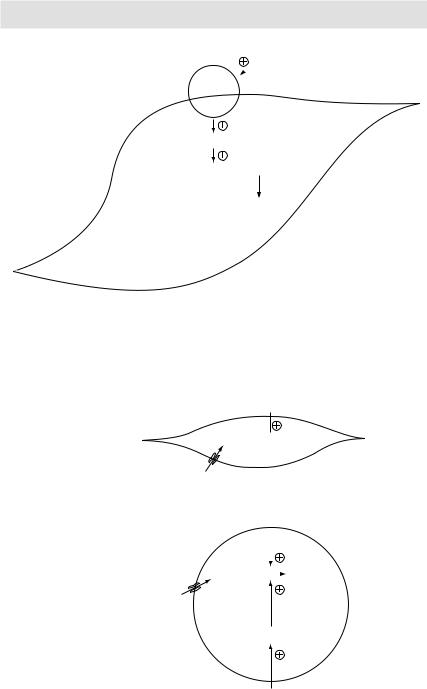
Ca++
↓intracellular Ca++
↓Ca++-Calmodulin complexes
↓Actin-Myosin crossbridges Relaxation
Myocyte
Figure 3.22 Mechanism of action of calcium channel blockers
|
|
K+-channel |
|
|
openers |
Ca++ |
K+ |
(minoxidil, nicorandil) |
Ca++ |
K+ |
|
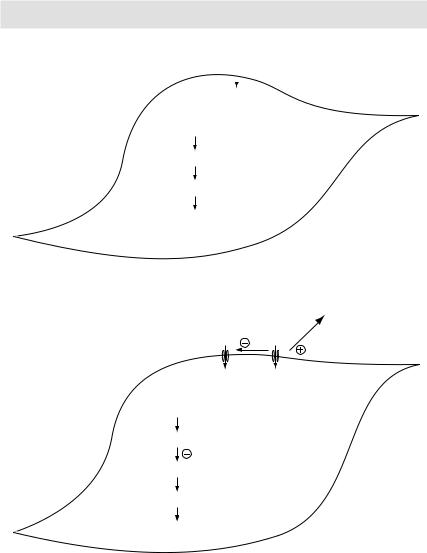
↑K+ efflux
Hyperpolarization
Ca++ channel opening
↓Ca++ influx
Myocyte Relaxation
Figure 3.23 Mechanism of action of K+-channel openers (minoxidil, nicorandil)
cIt causes the release of norepinephrine from adrenergic nerve endings via presynaptic AT1 receptor stimulation.
2Bradykinin to inactive metabolites. Bradykinin is one of the most potent vasodilators known. It acts via at least two receptors – β1 and β2.
Effects of ACE Inhibition: ACE inhibition decreases the concentration of angiotensin-II (a vasoconstrictor and stimulant for aldosterone release) and increases the concentration of bradykinin (a vasodilator). The net effect is a fall in blood pressure (with minimal compensatory responses), and K+ retention.
89
PHARMACOLOGY IN 7 DAYS FOR MEDICAL STUDENTS |
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Angiotensinogen |
|
|
|
|
|
|
|
|
|
|
|
|
Kininogen |
||||||||
|
|
|
(from liver) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Renin |
|
|
|
|
|
|
Inactive |
|
Kininase-II |
|
|
Kallikrein |
||||||||||||
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
metabolite |
|
|
|
|
|
|
|
|
Bradykinin |
||||
|
|
|
Angiotensin-I |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
ACE |
|
|
|
ACEIs |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
Vasodilatation |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
Angiotensin-II |
(from lungs) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
↓Peripheral |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
1. Vasoconstriction → ↑peripheral vascular |
|
|
|
|
|
|
|
vascular |
|||||||||||||
|
|
|
resistance |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
resistance |
||||
|
|
|
2. ↑thirst → ↑ADH release from posterior |
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
↓BP |
||||||||||||||
|
|
|
pituitary → ↑H2O absorption from collecting |
|
|
|||||||||||||||||||
|
|
|
tubules |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
↑BP |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
3. Aldosterone release from adrenal cortex → |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
↑Na+ and H2O reabsorption in exchange of |
|
|
|
|
|||||||||||||||||
|
|
|
H+ & K+ from distal convolated tubule |
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
4.↑Na+ and H2O reabsorption from the proximal |
|
|
|
|
|||||||||||||||||
|
|
|
convulated tubule by a direct action |
|
|
|
|
|
|
|
|
|
||||||||||||
Figure 3.24 Renin-angiotensin-aldosterone system |
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
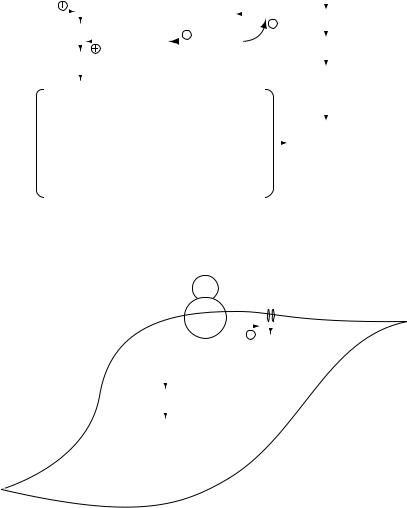
AT-II |
|
Ca++ |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
AT1 |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
receptor |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ca++ |
|
|
|
|
|||
|
|
|
|
|
|
|
AT1 receptor |
activation |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
↑intracellular Ca++ |
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
Contraction |
|
|
|
|
|
|
|
|
|
||||||||
Myocyte
Figure 3.25 Mechanism of angiotensin-II induced vasoconstriction
Angiotensin receptor blockers (ARBs)
As the name suggests ARBs competitively inhibit angiotensin-II from acting at AT1 receptors at adrenal cortex. They appear to be as effective as ACEIs in lowering the BP. Notably they do not block the conversion of bradykinin to inactive metabolites. Dry cough – a common side effect with ACEIs occurring in almost 30% cases – is due to a rise in the levels of bradykinin. Since ARBs lack this effect, they do not cause dry cough. In clinical practice, many patients who develop dry cough with ACEIs are switched to ARBs.
90
MECHANISMS OF ACTION
 Bradykinin
Bradykinin
Bradykinin
receptor
Endothelial nitric oxide synthetase
Arginine  Nitric oxide
Nitric oxide
Relaxation
Myocyte
Figure 3.26 Mechanism of bradykinin-induced vasodilatation
A
cell Muscle
Insulin
Glucose  Glycogen
Glycogen
B
Glucose
Insulin
|
|
|
|
|
ll |
|
|
|
|
|
|
|
e |
|
|
|
|
|
|
|
|
c |
|
|
|
|
|
|
|
|
e |
|
|
|
|
|
|
|
s |
|
|
|
|
|
|
|
o |
|
|
|
|
|
|
A |
d |
ip |
|
|
|
|
|
|
|
|
Glucose |
|
|
Triglyceride |
|||
|
|
|
|
|
||||
|
|
|
|
|
|
|||
|
|
|
|
|
|
|||
Glucose
PPARγ
Thiazolidinediones
Figure 3.27 A) Physiological action of insulin on muscle cells
B) Physiological action of insulin on adipose cells
91

PHARMACOLOGY IN 7 DAYS FOR MEDICAL STUDENTS
Since both ACEIs and ARBs cause K+ retention, concomitant use of these drugs with K+-sparing diuretics is not recommended lest toxic hyperkalemia should occur. Also, since both these groups of drugs damage the fetal kidneys, their use in pregnancy is absolutely contraindicated.
Sodium nitroprusside
Sodium nitroprusside is a short-acting (duration of action is a few minute), vasodilator always given as an intravenous infusion (never orally) in hypertensive emergencies. It produces its vasodilatory effect by causing the release of nitric oxide from the drug molecules itself, which in turn stimulates guanylyl cyclase and increases cGMP concentration in the smooth muscles.
Statins
Lovastatin and simvastatin are prodrugs; rest of the statins are active drugs. They inhibit hepatic synthesis of cholesterol by inhibiting an enzyme HMG-CoA reductase. 3-Hydroxy-3-methylglutaryl (HMG) is converted to mevalonate by an enzyme HMG-CoA reductase. This is the rate-limiting step in hepatic cholesterol biosynthesis. Statins by inhibiting HMG-CoA reductase in turn inhibit cholesterol biosynthesis leading to a fall in intracellular cholesterol concentration. Although cholesterol biosynthesis is blocked in other tissues as well, since statins undergo an extensive first-pass extraction, their primary effect is on liver. A fall in intracellular cholesterol concentration stimulates the synthesis of cell-surface LDL receptors. The resultant rise in the number of LDL receptors in turn causes an increased uptake of LDL cholesterol (the ‘bad’ cholesterol) from the blood. Statins thus reduce serum cholesterol levels by at least two mechanisms:
1↓ Hepatic cholesterol synthesis → ↓ hepatic cholesterol secretion into the blood.
2↑ LDL-cholesterol uptake from the blood.
The latter effect appears to be the more potent of the two in lowering serum cholesterol levels. Statins cause a rise in the level of HDL cholesterol (the ‘good’ cholesterol). The also decrease triglyceride levels.
Besides cholesterol-lowering effect, stains also have many other beneficial effects:
1Atheromatous plaque-stabilising effect.6
2Improvement in coronary endothelial function.
3Prevention of platelet aggregation.
4Anti-inflammatory effect.
5Prevention of bone loss.
FenoÞbrate
Fenofibrate is a prodrug. It is converted to an active metabolite ‘fenofibric acid’ which is responsible for the triglyceride-lowering effect of the drug. Fenofibric acid, once formed, attaches to its receptor: peroxisome proliferator-activated receptor-alpha
6Atheromatous plaques usually only partly fill the vascular lumen. Complete luminal obstruction (with resultant infarction and tissue death) usually occurs when part of the atheromatous plaque is ruptured by the blood stream followed by clotting of blood on the raw surface of the ruptured plaque. By ‘stabilising’ the plaque, statins reduce the risk of plaque rupture.
92

MECHANISMS OF ACTION
(PPAR-α). The activated receptor then binds to peroxisome proliferator response elements located in various gene promoters. These elements increase the expression of genes encoding for lipoprotein lipase. This enzyme is primarily found on the surface of endothelial cells. Its main function is to clip off free fatty acids from within the lipoprotein complexes so that the same can be taken up into the cells. This leads to depletion of triglycerides (3 × fatty acids + glycerol) from the lipoprotein complexes. Increased expression of lipoprotein lipase means increased clearance of triglyceriderich lipoproteins from the circulation leading to a fall in triglyceride levels. This also in turn leads to decreased cholesterol biosynthesis in the liver.
Fenofibrate also increases the level of HDL cholesterol (the ‘good’ cholesterol) by increasing the expression of two apolipoproteins apo A-I and apo A-II.
Insulin
Insulin synthesis: In the β-cells of the pancreas, insulin is initially synthesised as a prohormone called proinsulin (a single-chain polypeptide). It then undergoes proteolytic cleavage to form insulin (a two-chain polypeptide connected by disulfide bonds) and C-peptide, which are then secreted into the blood circulation. It is insulin that is responsible for all the physiological actions; neither proinsulin nor C-peptide appears to have any physiologic action.
Insulin secretion: A rise in blood glucose level, say after meals, causes increased glucose uptake by the β-cells of pancreas. Once inside the β-cells, glucose is metabolised. The products of glucose metabolism enter the mitochondrial respiratory chain generating ATP. A rise in ATP blocks K+ channels leading to membrane depolarisation and an influx of Ca++, which in turn causes insulin exocytosis. This explains a rise in insulin secretion following a rise in blood glucose level.
Box 3.2 Effects of insulin at target organs
Liver: |
¥ |
↑Glucose uptake |
|
¥ |
↑Glycogen synthesis |
|
¥ |
↓Glycogenolysis |
|
|
↓Gluconeogenesis |
|
¥ |
↓Protein catabolism |
Muscles: |
¥ |
↑Glucose uptake |
|
¥ |
↑Glycogen synthesis |
|
¥ |
↓Glycogenolysis |
|
|
↓Gluconeogenesis |
|
¥ |
↑Protein synthesis (insulin builds up muscle mass) |
Adipose tissue: |
¥ |
↑Glucose uptake |
|
¥ |
↑Triglyceride storage |
|
¥ |
↓Lipolysis (insulin builds up fat stores) |
Net effect of the above-mentioned actions is a fall in the blood glucose level.
Chloroquine
Plasmodium fulfils its need for essential amino acids by digesting the host cells haemoglobin. This process occurs in the food vacuoles of the organism and releases large amounts of heme, which is ordinarily toxic to plasmodium. The organism
93