Материал: surgical knot tying manual covidien
IV. components of a knotted suture loop using either a granny knot type or a square knot type
The mode of operation of a suture is the creation of a loop of fixed perimeter secured in the geometry by a knot.19
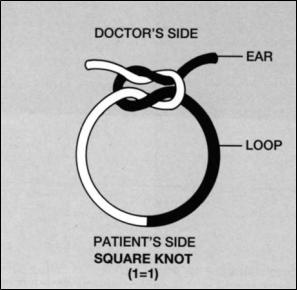
A tied suture has three components (Figure 1). First, the loop created by the knot maintains the approximation of the divided wound edges. Second, the knot is composed of a number of throws snugged against each other. A throw is a wrapping or weaving of two strands. Finally, the “ears” act as insurance that the loop will not become untied because of knot slippage. The doctor’s side of the knot is defined as the side of the knot with “ears,” or the side to which tension is applied during tying. The patient’s side is the portion of the knot adjacent to the loop.
22 |
Figure 1. The components of a tied suture. |
|
|
|
|
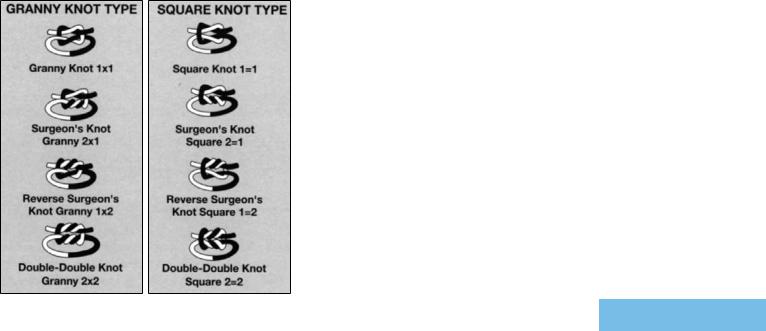
Each throw within a knot can either be a single or double throw. A single throw is formed by wrapping the two strands around each other so that the angle of the wrap equals 360°. In a double throw, the free end of a strand is passed twice, instead of once, around the other strand; the angle of this double-wrap throw is 720°. The tying of one or more additional throws completes the knot. The configuration of the knot can be classified into two general types by the relationship between the knot “ears” and the loop (Figure 2). When the right “ear” and the loop of the two throws exit on the same side of the knot or parallel to each other, the type of knot is judged to be square (reef). The knot is considered a granny type if the right “ear” and the loop exit or cross different sides of the knot.
When the knot is constructed by an initial double-wrap throw followed by a single throw, it is called a surgeon’s (friction) knot. The configuration of a reversed surgeon’s knot is a single throw followed by a double-wrap throw. A knot consisting of two double-wrap throws is appropriately called a double-double.
Figure 2. The configuration of surgical knots. |
23 |
|
IV. components of a knotted suture loop (cont’d)
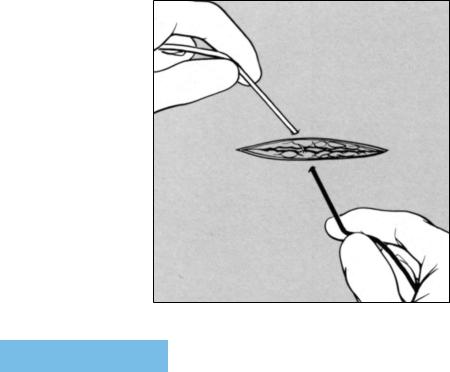
When forming the first throw of either a square or granny knot, the surgeon is merely wrapping one suture end (360°) around the other, with the suture ends exiting in opposite directions. The surgeon will apply equal and opposing tension to the suture ends in the same planes. The direction of the applied tensions will be determined by the orientation of the suture loop in relation to that of the surgeon’s hands. When the surgeon’s hands lie on each side and parallel to the suture loop, the surgeon will apply tensions in a direction parallel to his/her forearms. (Figure 3).
Figure 3. During knot construction, the surgeon’s hands should be on each side and parallel to the suture loop
24

Tension will be applied to the farther suture end in a direction away from the surgeon. Conversely, and equal opposing force will be applied to the closer suture end in a direction toward the surgeon. After constructing
the second throw of these knots, the direction of the suture ends must be reversed, with an accompanying reversal of the position of the surgeon’s hand. As the surgeon’s hands move toward or away from his body, the movements of his right and left hands are in separate and distinct areas that do not cross, permitting continuous visualization of knot construction. With each additional throw, the surgeon must reverse the position of his/her hands.
Orientation of the suture loop in a plane that is perpendicular to that of the surgeon’s forearms considerably complicates knot construction (Figure 4). In this circumstance, reversal of the position of the hands occurs in the same area, with crossing and overlapping of the surgeon’s hands, temporarily obscuring visualization of knot construction. This circumstance may be encountered when constructing knots in a
deep body cavity, which considerably limits changes in hand positions. This relatively cumbersome hand position may interfere with the application of uniform
opposing tensions to the suture ends, an invitation to the conversion of a square knot construction to a slip knot.
Figure 4. The surgeon’s hands frequently overlap (arrows) when the orientation of the hands is perpendicular to that of the suture loop.
25
IV. components of a knotted suture loop (cont’d)
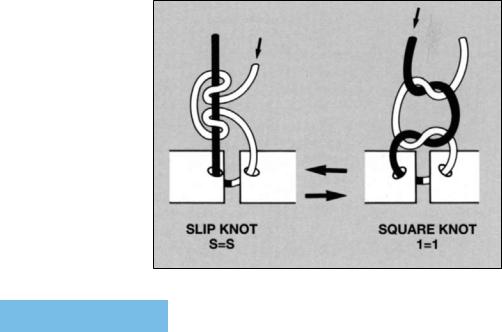
The granny knot and square knot can become a slip knot by making minor changes in the knot tying technique (Figure 5). Surgeons who do not reverse the position of their hands after forming each throw will construct slip knots. Furthermore, the application of greater tension to one ”ear” than the other encourages construction of slip knots, a practice commonly encountered in tying deep-seated ligatures.20
Figure 5. When the tension (arrow) is reapplied in equal and opposing directions, the slip knot can be converted into a square knot.
26