Материал: MasterPass _ Pharmacology in 7 Days for Medical Students
MECHANISMS OF ACTION
Tyrosine |
dopa-L |
Dopamine |
Reserpine |
MAO inhibitors |
|
Tricyclic |
antidepressants |
Noradrenaline |
Noradrenaline |
Noradrenaline |
|
|
m |
|
|
|
||
Dopamine |
Noradrenaline |
|
|
Noradrenaline |
|
receptor |
postsynaptic |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
c |
|
e |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
i |
|
|
|
m |
|
|
|
|
|
|
|
|
|
|
|
|
|
t |
|
|
|
b |
|||
|
|
|
|
|
|
|
|
|
|
|
p |
|
|
|
|
r |
||
|
|
|
|
|
|
|
|
|
|
|
a |
|
|
|
a |
|||
|
|
|
|
|
|
|
|
|
|
|
|
n |
|
|
|
n |
||
|
|
|
|
Degraded |
MAO by enzyme |
|
|
|
|
|
|
|
y |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
s |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
t |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
s |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
o |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P |
|
|
|
|
|
|
|
|
|
Ca++ |
Ca++ |
Noradrenaline |
receptor – |
presynaptic |
|
|
|
|
|
|
|
|
|
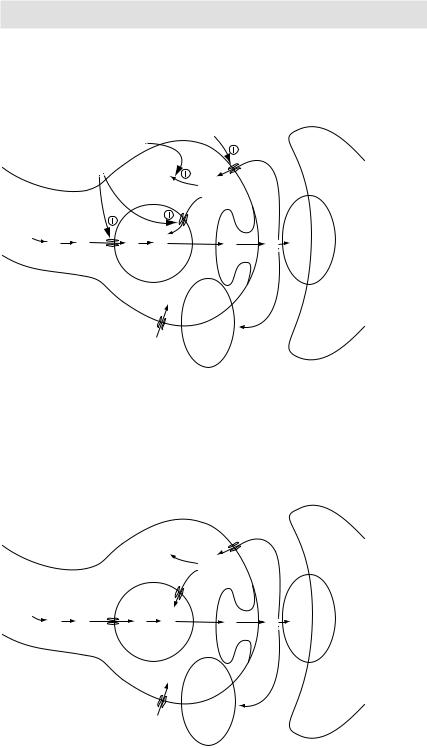
Noradrenergic neurotransmission: mechanism |
of action of reserpine, tricyclic antidepressants and MAOIs |
Figure 3.9 |
|
|
|
|
|
|
|
|
|
c |
m |
|
|
|
||
|
|
|
|
|
|
|
|
|
e |
|
|
|||
|
|
|
|
|
|
|
|
i |
|
|
|
m |
|
|
|
|
|
|
|
|
|
|
t |
|
|
|
|
b |
|
|
|
|
|
|
|
|
|
p |
|
|
|
|
r |
|
|
|
|
|
|
|
|
|
a |
|
|
|
a |
||
|
|
|
|
|
|
|
|
n |
|
|
|
n |
||
Tyrosine |
dopa-L |
Dopamine |
Dopamine by MAO |
Noradrenaline |
Noradrenaline |
Noradrenaline |
Noradrenaline |
postsynaptic |
|
e |
||||
Noradrenaline –receptor |
|
|
||||||||||||
|
|
|
Degraded |
enzyme |
|
|
|
y |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
s |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
t |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
s |
|
|
|
||
|
|
|
|
|
|
|
|
|
o |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
P |
|
|
|
|
|
|
|
Ca++ |
Ca++ |
Noradrenaline receptor – |
presynaptic |
|
|
|
|
|
|
|
|
Figure 3.8 Noradrenergic neurotransmission
69
PHARMACOLOGY IN 7 DAYS FOR MEDICAL STUDENTS
Tryptophan |
Serotonin |
Reserpine |
Degraded |
Serotonin |
enzyme |
Serotonin antidepressants Serotonin |
receptor inhibitors |
Serotonin |
Serotonin |
–receptor |
postsynaptic |
|
|
|||
|
|
|
|
inhibitors MAO |
|
Tricyclic |
serotonin selective & |
|
c |
|
e |
|
|
|||
|
|
|
|
|
|
|
|
|
|
i |
|
m |
m |
|
||
|
|
|
|
|
|
|
|
|
|
t |
|
|
|
b |
||
|
|
|
|
|
|
|
|
|
|
p |
|
|
|
|
r |
|
|
|
|
|
|
|
|
|
|
|
a |
|
|
|
a |
||
|
|
|
|
|
|
|
|
|
|
n |
|
|
|
n |
||
|
|
|
|
MAO |
|
|
|
|
|
|
|
|
e |
|||
|
|
|
|
|
|
|
|
|
|
y |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
s |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
t |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
s |
|
|
|
||
|
|
|
|
by |
|
|
|
|
|
|
o |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
P |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Na+ |
Ca++ |
Serotonin receptor – |
presynaptic |
|
|
|
|
|
|
|
|
|
|
|
|
Na+ |
Ca++ |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
c |
m |
|
|
|
||
|
|
|
|
|
|
|
|
|
e |
|
|
|||
|
|
|
|
|
|
|
|
i |
|
|
|
m |
|
|
|
|
|
|
|
|
|
|
t |
|
|
|
b |
||
|
|
|
|
|
|
|
|
p |
|
|
|
|
r |
|
|
|
|
|
|
|
|
|
a |
|
|
|
a |
||
|
|
|
|
|
|
|
|
n |
|
|
|
n |
||
|
|
Degraded |
MAO |
enzyme |
|
|
|
|
|
|
e |
|||
|
|
Serotonin |
|
|
|
y |
|
|
|
|
||||
Tryptophan |
Serotonin |
Serotonin |
Serotonin |
Serotonin |
|
postsynaptic |
|
|
||||||
Serotonin –receptor |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
s |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
t |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
s |
|
|
|
||
|
|
|
by |
|
|
|
|
|
o |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
P |
|
|
|
|
|
|
|
Na+ |
++ |
|
|
|
|
|
|
|
|
|
|
|
|
Na+ |
Ca++ |
Ca |
Serotonin receptor – |
presynaptic |
|
|
|
|
|
|
|
|
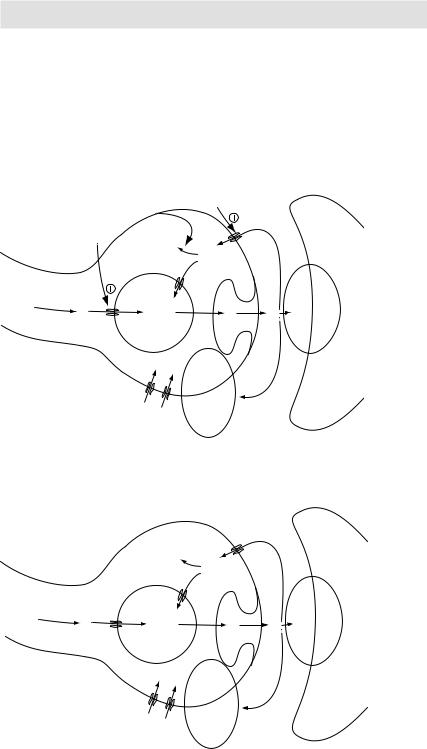
Figure 3.10 Serotonergic neurotransmission Figure 3.11 Serotonergic neurotransmission: mechanism of action of reserpine, MAOIs, TCAs and SSRIs
70

MECHANISMS OF ACTION
3Also, because they unmask the manic behaviour, they should be cautiously used in manic-depressive patients.
Selective serotonin re-uptake inhibitors (SSRIs)
As the name suggests these drugs block the pre-synaptic re-uptake of the serotonin with resultant greater post-synaptic neuronal activity. Unlike TCAs, which block the reuptake of both serotonin (5HT) and noradrenaline (by blocking 5HT and α2 presynaptic receptors respectively), SSRIs have 300to 3000-fold greater selectivity for 5HT receptors and thus primarily block the re-uptake of serotonin. Also, they have little ability to block the dopaminergic, muscarinic, α-adrenergic and histaminic (H1) receptors. Because of this, SSRIs lack many of the side effects commonly encountered with TCA therapy, e.g. sedation, blurred vision, dry mouth and orthostatic hypotension. Fewer side effects, and being relatively safe even in high doses, have made SSRIs the drug of choice in most patients of depression in preference to TCAs and MAOIs.
SSRIs do not produce CNS stimulation or mood elevation in healthy subjects.
Monoamine oxidase inhibitors (MAOIs)
Monoamine oxidase (MAO) is a mitochondrial enzyme found in the neurons (and other tissues such as gut and liver). In the neurons, MAO functions as a safety valve to oxidatively deaminate and thus inactivate any excess neurotransmitter molecules (serotonin, noradrenaline and dopamine) that may leak out of the synaptic vesicles when the neuron is at rest. MAOIs may irreversibly or reversible inactivate both monoamine oxidase enzymes (MAO-A and MAO-B) by forming a strong covalent bond with the active sites of these enzymes. This results in inhibition of intraneuronal degradation of serotonin, noradrenaline and dopamine with resultant increase in the vesicular stores of these amines. When neuronal activity discharges the vesicles, increased amounts of the amines are released in the synaptic cleft causing enhanced activation of serotonin, noradrenaline and dopamine receptors. This may be responsible for the antidepressant actions of MAOIs. Notably, these MAOIs do not affect the synthesis and reuptake of the said amines.
MAOIs not only inhibit MAO in the brain, but also peripheral oxidases that catalyse oxidative deamination of drugs and potentially toxic substances such as tyramine, which is found in certain foods. MAOIs therefore show a high incidence of drug–drug and drug–food interactions.
Two MAOIs currently available for the treatment of depression are phenelzine and tranylcypromine. Besides inhibiting MAO, both these drugs show a direct (though mild), amphetamine-like stimulant effect. This makes theses drugs the preferred choice in depressed patients with low psychomotor activity. Also, they are indicated in depressed patients with associated severe anxiety, patients who are unresponsive or allergic to TCAs and patient’s suffering from phobias or atypical depression.3
Levodopa
Since Parkinsonism results from dopamine deficiency in specific regions of the brain, attempts have been made to replenish the deficient dopamine.
3Atypical depression is characterised by labile mood, appetite disturbances and rejection sensitivity.
71

PHARMACOLOGY IN 7 DAYS FOR MEDICAL STUDENTS
Levodopa is rapidly absorbed from the small intestine (when empty of food), crosses BBB actively4 and reaches nigrostriatal pathway5. It is taken up by substantia nigra and converted there into dopamine by cerebral dopa decarboxylase. Dopamine is released from N-terminal into striatal area thus making up dopamine deficiency and restoring the balance between dopamine and acetylcholine. This helps control the manifestations of Parkinsonism.
Large doses of levodopa are required because much of the drug is decarboxylated to dopamine in GIT and peripheral tissues resulting in side effects (like N, V, cardiac arrhythmias and hypotension). The effects of the levodopa on the CNS can be greatly enhanced by coadministering carbidopa (dopa decarboxylase inhibitor that does not cross the BBB). Carbidopa diminishes the metabolism of levodopa in the GIT and peripheral tissues hence increasing the CNS availability of levodopa. Addition of carbidopa lowers the doses of levodopa required by 4- to 5-folds and also decreases the severity of side effects of peripherally formed dopamine.
Levodopa has an extremely short half-life of 1–2hrs, which causes fluctuations in plasma concentration. This may produce fluctuations in motor response (on-off phenomenon), which may cause sudden worsening of the previously controlled Parkinsonian symptoms (loss of normal mobility, rigidity, tremors, and cramps).
Note that although levodopa meets dopamine deficiency in the brain, it does not stop the loss of dopaminergic neurons in the nigrostriatal pathway. This loss continues unchecked as the disease progresses so that after a given time very few dopaminergic neurons are left intact to take up levodopa for onward conversion to dopamine. Thus although levodopa produces a remarkable improvement in the symptoms during the initial period of therapy, its overall therapeutic efficacy declines with time.
Ingestion of meals particularly if high in protein content interferes with the transport of levodopa into the CNS. Large neutral amino acids, e.g. leucine and isoleucine compete with levodopa for absorption from the gut and for transport across the BBB. Thus levodopa should be taken on an empty stomach, typically 45 minutes before a meal.
Withdrawal from the drug must be gradual.
Penicillins
As antibacterial drugs, mechanism of action of all penicillins is the same. Penicillins are bactericidal and act by inhibiting the cell wall synthesis of the susceptible bacteria by blocking transpeptidation/cross links between the peptidoglycan chains through the inhibition of the enzymes transpeptidases. This renders the cell walls very weak resulting in loss of its protection to inner cytoplasmic membrane of the bacteria, which then bulges out under the high intracellular osmotic pressure and finally bursts out throwing its contents, i.e. essential macromolecules outside the cell. Thus death/ lysis of bacterial cells occur.
Penicillins cause activation of autolysins by removing autolysin inhibitors. Autolysins on becoming active start destroying the bacterial cell wall. In order to inhibit transpeptidases, penicillins have to reach their targets, i.e. penicillins binding proteins (PBP) located on inner cytoplasmic membranes. They enter through the hydrophilic poring
4 Dopamine itself does not cross the BBB.
5Nigrostriatal pathway is the extrapyramidal center where most dopaminergic neurons are concentrated. In Parkinsonism, dopaminergic neurons are partly lost, resulting in atrophy of the nigrostriatal pathway.
72
MECHANISMS OF ACTION
|
Tyrosine |
|
|
|
L-dopa |
|
|
|
Dopamine |
|
|
|
Dopamine |
Degraded |
|
Ca++ |
by MAO |
||
(in secretary |
|||
|
enzyme |
||
Ca++ |
vesicles) |
||
|
|||
Dopamine |
|
Dopamine |
|
receptor – |
|
||
presynaptic |
Dopamine |
|
|
|
|
Dopamine
Dopamine receptor – postsynaptic
|
|
|
|
|
|
|
ti |
||
|
|
|
|
|
pc |
||||
|
|
|
|
a |
|
|
|
|
|
|
|
|
n |
|
|
|
|
|
|
|
|
y |
|
|
|
|
|
|
|
|
ts |
|
|
|
|
|
|
|
|
s |
|
|
|
|
|
|
|
|
|
Po |
|
|
|
|
|
|
|
|
m |
|
|
|
|
|
|
|
b |
m |
e |
|
|
|
|
|
|
r |
|
||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a |
|
|
|
|
|
|
|
|
n |
|
|
|
|
|
|
|
|
e |
|
|
|
|
|
|
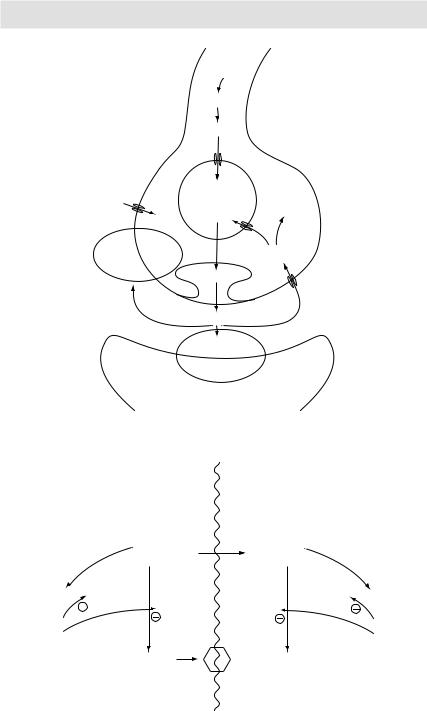
Figure 3.12 Dopaminergic neurotransmission
3-O-MD
Entacapone
Carbidopa
Metabolized |
||
|
by |
COMT |
|
|
|
|
|
|
L-dopa in |
BarrierBrain Blood |
L-dopa |
|
periphery |
in brain |
Metabolized |
Metabolized |
by AADC |
by MAO-B |
byMetabolized COMT
3MT
Tolcapone
Selegiline
Dopamine |
Stop |
DOPAC |
Figure 3.13 Mechanism of action of levodopa and other anti-Parkinsonism drugs
73