Материал: MasterPass _ Pharmacology in 7 Days for Medical Students

CLASSIFICATIONS
• Sodium nitroprusside
Therapeutic classiÞcation of anti-epileptic drugs
ADrugs used in partial (focal) epilepsy
1For simple partial epilepsy
•Lamotrigine
•Felbamate
•Phenytoin
•Carbamazepine
•Primidone
•Gabapentin
•Vigabatrin
•Topiramate
2For complex partial/psychomotor/temporal-lobe epilepsy and Jacksonian epilepsy
•Phenytoin
•Carbamazepine
•Primidone
•Gabapentin
•Vigabatrin
•Topiramate
BDrugs used in generalised epilepsy
1For grand-mal epilepsy/generalised tonic-clonic seizures
•Sodium valproate
•Phenobarbitone
•Primidone
•Gabapentin
•Vigabatrin
•Lamotrigine
•Felbamate
2Petit-mal epilepsy/absence seizures
•Sodium valproate
•Clonazepam
•Ethosuximide
3Atonic seizures
•Sodium valproate
•Clonazepam
•Nitrazepam
4Myoclonic seizures
•Clonazepam
5Febrile seizures (in children)
•Phenobarbitone
•Primidone
6Infantile spasms
•Corticotropin
•Vigabatrin
•Nitrazepam
49

PHARMACOLOGY IN 7 DAYS FOR MEDICAL STUDENTS
7Status epilepticus
•Diazepam
•Fosphenytoin
•Thiopentone sodium
•Phenobarbitone
Therapeutic classiÞcation of benzodiazepines
1Sedative/hypnotics
•Flurazepam
•Nitrazepam
•Triazolam
•Lormetazepam
2Anxiolytics
•Diazepam
•Lormetazepam
•Oxazepam
3Anticonvulsants
•Diazepam
•Clonazepam
•Nitrazepam
4Central muscle relaxants
•Diazepam
•Clonazepam
•Flurazepam
50
3
Mechanisms of action
Reversible anticholinesterases
Drugs included: neostigmine, physostigmine, edrophonium and echothiophate. Acetylcholine released in the synaptic cleft is degraded into acetate and choline
by an enzyme acetylcholinesterase thus terminating its action. This enzyme is found bound to both preand postsynaptic membranes. Anticholinesterases inhibit this enzyme thus blocking acetylcholine degradation and prolonging its action. These drugs stimulate all acetylcholine receptors in the body, i.e. muscarinic and nicotinic receptors of ANS, nicotinic receptors present at NMJ and CNS cholinoceptors.
1Physostigmine: It is a reversible anticholinesterase. Chemically it is a carbamic acid ester and a substrate for acetylcholinesterase. The action of acetylcholinesterase on this drug results in the formation of a relatively stable carbamoylated intermediate with the enzyme, which thus becomes inactive. This in turn leads to prolongation of acetylcholine action on cholinoceptors throughout the body. The duration of action of physostigmine is about 2–4 hours.
2Donezepil, Rivastigmine and Galantamine: These drugs are also reversible anticholinesterases and are primarily used in the treatment of Alzheimer’s disease. The basic pathology in Alzheimer’s disease is a deficiency of cholinergic neurons in the CNS. By inhibiting acetylcholinesterase enzyme and thus acetylcholine degradation these drugs try to overcome the deficiency of cholinergic neurons in the brain. Studies have shown that these drugs do slow the progression of Alzheimer’s disease, but only for a time being. The main side effect of these drugs is GI upset.
Irreversible anticholinesterases
Drugs included: It includes organophosphate compounds like isoflurophate, parathion, etc. Chemically these drugs are organophosphorous compounds. Their mechanism of action is similar to other anticholinesterases; the only difference is that these agents covalently bind to acetylcholinesterase, thus permanently and irreversibly inactivating it so that reactivation of acetylcholinesterase activity requires the synthesis of new enzyme molecules. The net result is a long-lasting increase in the cholinergic activity throughout the body (↑ lacrimation, salivation, sweating, miosis, NVD, etc.), motor paralysis (→ breathing difficulty) and convulsions. Owing to such toxic effects these drugs have been developed for military use as nerve agents. The prototype amongst
these is isoflurophate.
Isoflurophate: This organophosphorous compound covalently binds with the enzyme anticholinesterase thus inhibiting it permanently. Anticholinesterase activity is
51

PHARMACOLOGY IN 7 DAYS FOR MEDICAL STUDENTS
restored only once new enzyme molecules are synthesised by the body.
Acetylcholinesterase reactivators (pralidoxime): Since the human body on its own cannot cleave the covalent bond between anticholinesterase enzyme and isoflurophate, the enzyme inactivation is permanent. However, scientists have developed chemical reactivators such as pralidoxime, which, if given within the first few hours of nerve agent exposure, can cleave this covalent bond, thus causing anticholinesterase reactivation and correction of muscle paralysis, breathing difficulties and convulsions. The only shortfall of anticholinesterase reactivators is that these agents are effective only before ‘aging’ has occurred. ‘Aging’ refers to the phenomenon of release of one of the alkyl groups by the anticholinesterase-isoflurophate moiety. Once an alkyl group is lost (i.e. aging has occurred), even chemical reactivators like pralidoxime also become ineffective, i.e. they can no longer cleave the covalent bond between anticholinesterase and isoflurophate. Isoflurophate ages in 6–8 hours. Thus, to be effective, it is necessary that pralidoxime is given within this period. The newer nerve agents, available to the military, age within minutes or even seconds.
Antidote of irreversible anticholinesterases: Atropine, by inhibiting antimuscarinic receptors, acts as an antidote of irreversible anticholinesterases. Until the body synthesises new molecules of anticholinesterase enzyme, we can use atropine (in high doses) to block many of the muscarinic and central effects of isoflurophate.
Castor oil
It is a stimulant laxative. In the small intestine, it is broken down to ricinoleic acid, which increases intestinal peristaltic activity, thus relieving constipation. Exaggerated peristaltic activity can produce abdominal cramps. Protracted use of stimulant laxatives is not advisable as they can cause atonic colon with prolonged use.
Cascata, senna and aloe are other agents, which are used as laxatives. These contain emodin – the principal agent that stimulates colonic peristaltic activity. These agents are first absorbed in the small intestine and later excreted into the colon. The onset of action of these agents is thus delayed by 6–8 hours. This delay is, in fact, beneficial because one tablet of senna taken at bedtime causes bowel movement not before early in the morning.
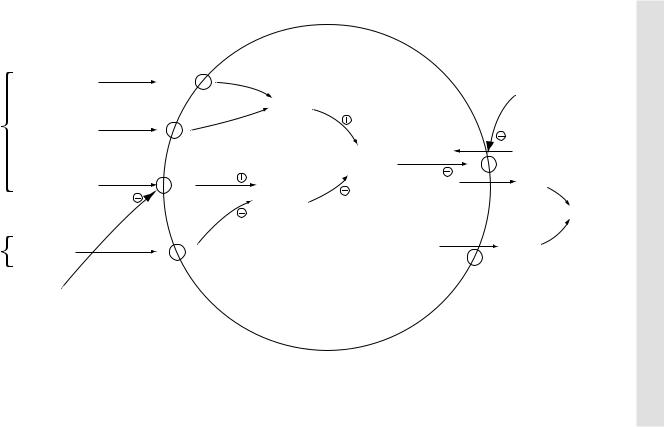
Regulation of gastric HCl secretion
Gastric HCl is produced and secreted by parietal cells. Acetylcholine, histamine and gastrin stimulate parietal cells whereas prostaglandin E2 and somatostatin inhibit them. Parietal cells have membrane receptors for all these agents.
When stimulants attach with their respective receptors, there occurs activation of protein kinases. Histamine initially causes activation of adenylyl cyclase enzyme, which in turn causes activation of protein kinases. Acetylcholine and gastrin, however, cause Ca++ influx. This in turn causes a rise in intracellular Ca++ levels and activation of protein kinases. Protein kinases in turn activate the H+/K+-ATPase proton pump. This pump actively secretes one H+ ion into the gastric lumen in exchange for one K+ ion pumped into the parietal cell from gastric lumen. Additionally, one Cl– ion is secreted from the parietal cell into the gastric lumen via a separate Cl– channel. Within the gastric lumen H+ and Cl– join to form HCl.
When inhibitors like prostaglandin E2 bind with their respective receptors, there occurs inactivation of adenylyl cyclase enzyme. This in turn causes inactivation of protein kinases and H+/K+-ATPase proton pump thus inhibiting HCl formation.
52
|
Gastrin |
|
Gastrin |
Parietal |
receptor |
|
|
cell |
Acetylcholine |
stimulants |
ACh |
|
|
|
receptor |
|
Histamine |
|
Histamine-2 |
|
receptor |
Parietal |
PGE2 |
cell |
|
inhibitor |
PGE2 |
|
Receptor |
|
H2 receptor |
|
blockers |
PPI
↑Ca++
Protein |
K+ |
|
K+/H+ |
|
|
kinase |
ATPase |
H+ |
|
||
Adenylyl |
pump |
|
cyclase |
|
HCl |
|
|
|
|
Cl– |
|
|
Chloride |
|
|
channel |
|
P |
l l |
arietal c e |
|
Figure 3.1 Regulation of gastric HCl secretion in parietal cells
53
ACTION OF MECHANISMS