Материал: Internal_diseases_propedeutics._Part_II._Diagnostics_of_cardiovascular_diseases
The heart auscultation: heart murmurs
Cardiac murmurs are relatively long lasting sounds appearing during turbulent blood motion. The turbulence appears in case of disturbance of three hemodynamic parameters normal proportion:
1.Diameter of valve ostium or vessel lumen;
2.Blood flow velocity (linear or volume);
3.Blood viscosity.
Murmurs heard above the region of the heart and large vessels are divided into intraand extracardiac.
Intracardiac murmurs.
Intracardiac murmurs are divided into:
1.organic, appearing due to rough organic lesion of valves and other cardiac anatomic structures (interventricular or interatrial septum);
2.functional murmurs based not on rough anatomic structures lesions, but on lesion of valvular functions, blood flow acceleration through anatomically unchanged ostiae or blood viscosity decrease.
Organic murmurs: all the organic intracardiac murmurs appear in presence of narrowing, dilation or other obstacles, for example, parietal thrombus or atherosclerotic patch on aortic wall in cardiac cavities or initial parts of main vessels.
One should give its detailed characteristic, namely, define:
1.murmur relation to cardiac activity phases (systolic, diastolic, etc.) (Fig. 20, 21);
2.region of maximal murmur intensity;
3.murmur transmission;
4.timbre, volume of the murmur;
5.shape of murmur.
For more information look at tables 3,4
36
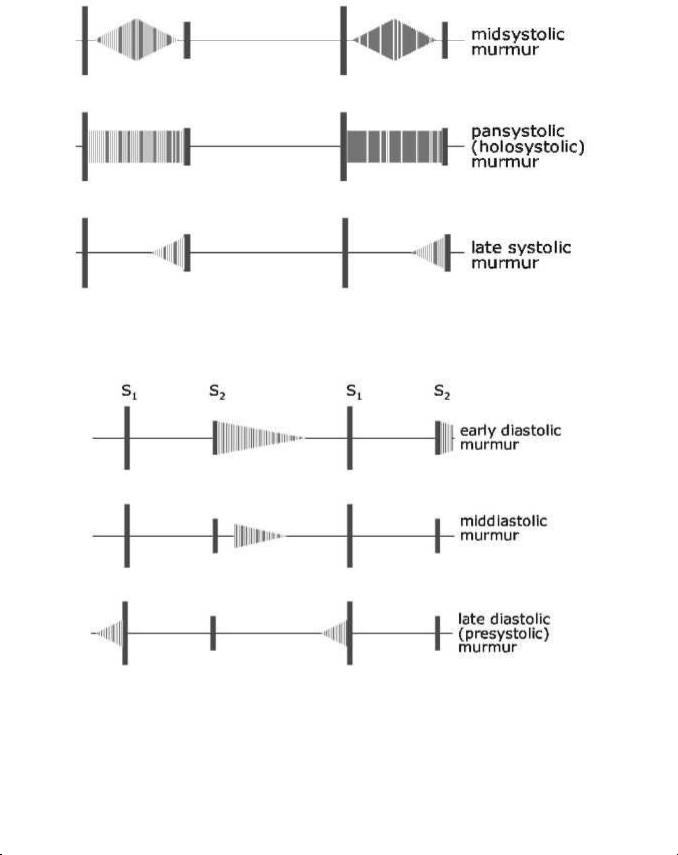
Fig. 20. Main types of systolic murmurs.
Fig. 21. Main types of diastolic murmurs.
Table 3.
Chief systolic murmurs
Time and quality |
Accompanying signs |
|
Interpretation |
|
|
|
|
1. Ejection, harsh midsystolic |
Slow rising pulse, low |
systolic pressure, |
Aortic stenosis |
accentuation or prolonged |
heaving apex beat, systolic thrill, ejection click, |
|
|
|
|
|
|
|
37 |
|
|
|
|
|
|
|
|
|
soft or absent A2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
2. |
Ejection, as above. Loudest |
Jerky pulse, atrial impulse over |
apex, |
lifting |
Hypertrophic |
obstructive |
|||||||||
in left 3rd, 4th interspace |
|
|
apex beat |
|
|
|
|
|
|
cardiomyopathy |
|||||
|
|
|
|
|
|
|
|
|
|||||||
3. Ejection, as above |
|
|
Hyperkinetic |
states, |
aortic |
incompetence, |
Increased flow |
||||||||
|
|
|
|
|
|
|
complete heart block |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
4. Ejection, as above |
|
|
No signs |
|
|
|
|
|
|
Aortic stenosis |
|||||
|
|
|
|
|
|
|
|
|
|
|
|||||
5. |
Ejection, |
over |
pulmonary |
Increases during inspiration |
|
|
|
|
Pulmonary stenosis |
||||||
area |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
6. |
Ejection, |
short, |
over |
Hyperkinetic states, left-to-right |
|
shunt |
(ASD, |
Increased flow |
|||||||
pulmonary area |
|
|
|
VSD) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
7. |
Late |
ejection, |
over |
mitral |
Mid-systolic click |
|
|
|
|
|
Mitral valve prolapse |
||||
area |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
8. |
Pansystolic, |
blowing, |
Large volume |
pulse, |
displaced |
and vigorous |
Mitral incompetence |
||||||||
mostly uniform |
|
|
|
apex, right ventricular heave, S3, louder during |
|
|
|||||||||
|
|
|
|
|
|
|
expiration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
9. |
Pansystolic, as above. Best |
As above plus thrill frequently presents |
|
Ventricular septal defect |
|||||||||||
heard |
over |
left |
|
3rd, |
|
|
|
|
|
|
|
(VSD) |
|
||
4th interspace |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Table 4. |
|
|
|
|
|
|
|
Chief diastolic murmurs |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|||||||
Time and quality |
|
|
Accompanying signs |
|
|
|
Interpretation |
|
|||||||
|
|
|
|
|
|
||||||||||
1. |
Early diastolic, high- |
Collapsing pulse, Corrigan's sign, |
wide |
Aortic incompetence |
|
||||||||||
pitched, blowing |
|
|
pulse pressure, displaced and vigorous |
|
|
|
|
||||||||
|
|
|
|
|
|
apex |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
2. |
Early diastolic, |
a short, |
Prominent 'a' wave, right ventricular heave |
Graham |
Steell |
murmur |
|||||||||
high-pitched whiff |
|
|
loud P2 |
|
|
|
|
(functional |
pulmonary |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
incompetence) |
|
||
|
|
|
|
|
|
||||||||||
3. |
Mid-diastolic, |
rough, |
Malar flush, small volume pulse, tapping |
Mitral stenosis |
|
||||||||||
rumbling |
|
|
|
|
impulse, right ventricular heave, opening |
|
|
|
|
||||||
|
|
|
|
|
|
snap |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
4. |
Mid-diastolic, |
short,Signs of mitral |
incompetence, VSD |
orInflow (mitral) murmur |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
38 |
|
|
|
|
|
|
|
following S3 |
|
paten t ductus |
|
|
|
|
|
|
|
|
|
|
|
5. |
Mid-diastolic, |
short, |
Sign s of atrial septal defect (ASD) |
|
Inflow |
(tricuspid) murmur |
over tricuspid area |
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
Continuous systolic and |
Colla psing pulse, thrill, mitral |
inflow |
Patent |
ductus, aortopulmonary |
|
diastolic, machinery noise |
murm ur |
|
septal defect |
|||
|
|
|
|
|
|
|
Examples of most cha racteristic murmurs in five acquired cardiac defects: mitral incompetence, mitral stenosi s, aortic stenosis, tricuspid incompete nce.
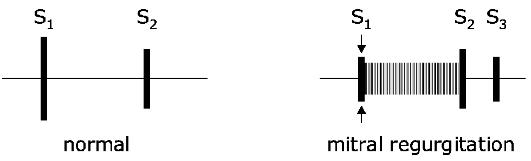
Mitral incompetence is characterized by diminished S1, systo lic murmur appearance and S2 accent at the pulmon ary artery. On PhonoCG decrease of S1 amplitude is marked in significant mitral incompetence due to falling out of S1 v alvular component and overfilling of left ventricle. Minor degree of mitral incompetence isn't accompanied by S1 diminishing. The most imp ortant in mitral incompetence diagn ostics is a presence of systolic murmur with maxi mal intensity at the apex (Application Fig.2). In severe valve disease murmur of considera ble intensity is registered at the left ax illa. Systolic murmur is directly connected with def ect, formed between valve leaflets a nd reverse blood flow (regurgitation) through this chink. Murmur in mitral incompetence begins directly after S1 and has decrescent character. It may occupy all systole (pansy stolic) or part of systole according to the degree of mitral incompetence. Murmur amplitude is more when the defect is pronounced (Fig. 2 2).
Fig. 22. When the mitr al valve fails to close fully in systole, blood regurgitates from left ventricle to left atrium, causing a murmur. S1 is often decrease d. An apical S3 reflects the volume overload on the l eft ventricle.
39
At the pulmonary artery increase of S2 pulmonary compone nt (P2) is noticed, S2 is frequently splitted.
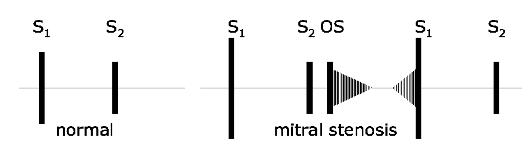
Mitral stenosis: Since a little amount of blood gets into left ventricle and it contracts fast, so S1 at the apex beco mes loud, flapping. Here after S2 the a dditional heart sound – mitral opening snap – is listened. Flapping S1, S2 and openin g snap (OS) create the typical of mitral stenosis m elody called ―quail rhythm (Fig.23). A rumbling diastolic murmur at the apex is typical of mitral stenosis, because there is narrowing down blood flow from the left atrium to the left ventricle on diastole (Application Fig.1). This murmur may occur in the very beginning of diastole, i.e. to be protodiastolic, because due to pressure gradient in atrium and ventricle the blood flow velocity will be higher at the diastole beginning. However, murmur appears only at the end of diastole before the very systole – presystolic murmur, which appears in blood flow acceleration at the end of diastole due to atrial contra ction. There may be presystolic accen tuation and the murmur may be preceded by an opening snap. Exercise and positioning the patient in the left lateral position will accentua te the murmur (Fig.22).
Fig. 23. When the leaflets of the mitral valve thicken, stiffen, and become distorted, the valve fails to open suffic iently in diastole. The resulting murmur has two components: mid-diastolic (during rapid ventricular filling), and presystolic (du ring atrial contraction). S1 is accentuated. An openin g snap (OS) often follows S2 and initia tes the murmur.
As pulmonary hypertension develops, the pulmonary s econd sound becomes accentuated.
Aortic incompetence: o n auscultation diminished S1 at the ap ex is revealed, because during systole there is no pe riod of closed valves. S2 at the aorta is also diminished, and
40