Материал: Internal_diseases_propedeutics._Part_II._Diagnostics_of_cardiovascular_diseases

Fig.13"Spherical” configuration of the heart. in a patient with a congenital heart defect. The chest radiograph of a patient with a ventricular septal defect (direct view): the shadow of the heart increased at the expense of both ventricles, visible bulging arc pulmonary trunk (arrow), pulmonary picture in the basal parts of the lungs are strengthened.
"Drip" configuration of the heart - the left and right border of cardiac dullness is shifted medially, the area of cardiac dullness is diminished, the heart becomes "drip" form, cause - emphysema of the lungs (Fig.14).
26
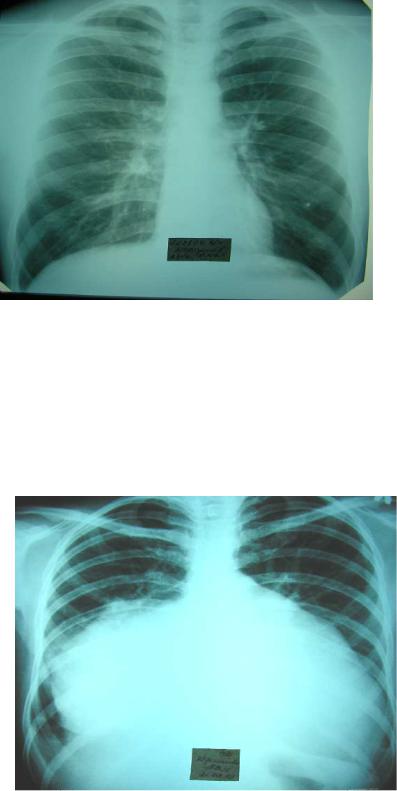
Fig.14. "Drip" configuration of the heart
"Cor bovinum" ("bu ll" heart) - the area of cardiac du llness is increased by hypertrophy and/or dilatatio n of its main offices in cardiomyopathy, advanced forms of heart failure.
Fig.15. "Cor bovinum"
27
Auscultation of the heart and blood vessels.
Auscultation points of the heart valves do not coincide with the projection places of the valves on the anterior chest wall (only pulmonic valve auscultation point practically coincides with the projection of the pulmonary artery valve).
Places of three heart valves projection - pulmonary, aortic and mitral - are located very close to each other, about the place of the III rib attachment to the sternum (therefore to distinguish particular sounds associated with damage of each of these valves, when listening to their places of projection is not possible). The diameter of the valves openings is large enough and is 2-3 cm for pulmonary, aortic and mitral valves and 3-6 cm for tricuspid valve. Therefore, in determining the projection of the heart valves it must be taken into account their length, as projection of the valve is not the point, but rather the line of few centimeters.
The surface projections of the heart valves on the anterior chest wall (approximately) are as follows (Fig. 16):
1.The pulmonic valve is located at the place of attachment of the upper edge of III left costal cartilage to the sternum (1/2 portion of the valve is located behind the rib cartilage, 1/2 part of the valve-behind the sternum).
2.Aortic valve is located just medially, slightly lower and deeper than pulmonary valve - almost in the middle of the sternum at the level of the III mid-rib.
Bicuspid (mitral) and tricuspid atrioventricular valves are located behind the sternum in the arcuate line connecting places of the lower part of the left III rib cartilage and the right V-VI costal cartilages attachments to the sternum.
3.Bicuspid (mitral) valve is located within the limits of upper third of this line and is located in between the attachment place of the lower edge of the III rib cartilage to the sternum and the level of the third left intercostal space.
4.Tricuspid valve is within the limits of lower 2/3 of this line and is located in between the level of the left third intercostal space and the attachment point of the right V costal cartilage to the sternum (in fact, in the lower part of the sternum body).
28
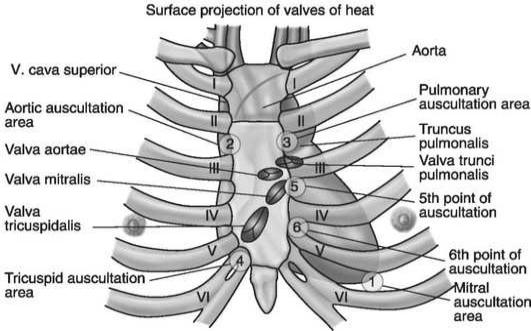
Fig. 16. Projection of the heart valves on the anterior chest wall and their auscultation points
Since all the heart valves are located close to each other, to evaluate the sound effects associated with the work of each valve there are used more remote points from the valves location, where the sound is carried either by the flow of blood, or by myocardium of the heart area, where this sound is produced and where the summation of the sounds originating in neighboring parts of the heart is minimal.
There are distinguished the 6 heart auscultation points: 4 main and 1 additional points.
«Assignment» numbers to the auscultation points (1st auscultation point, 2nd auscultation point, etc.) and listening to the heart valves in this sequence in clinical practice is determined by the frequency of their damage (i.e. the most frequently damaged mitral valve, and most rarely - tricuspid one).
1. The first auscultation point - region of the apical impulse (normally - the V intercostal space slightly medially from l. medioclavicularis sinistrum, in the pathology, apical impulse may be displaced considerably from its location in the norm). At this point, mitral (bicuspid) valve is well heard. This is because in its projection (behind sternum at the level of the lower edge of the III rib cartilage - 3rd intercostal space) mitral valve is rather deeply spaced apart from the chest wall (i.e. the sounds from it are not properly
29
heard), and at the apex of the heart, which is formed by the left ventricle, mitral valve
sounds are well conducted by dense heart muscle.
2.The second auscultation point-2nd right intercostal space close to the sternum. This point is a place of the aortic valve auscultation. As mentioned above, the aortic valve is projected on mid-sternum at the level of the III rib middle, but it is common to listen to the aorta in the right 2nd intercostal space, because aorta here comes close to the anterior chest wall and here aortic valve sounds are well conducted along by the flow of blood and the wall of the aorta.Therefore, when listening to the right 2nd intercostal space, one can be sure that the sounds and murmurs belong exactly to the aortic valve.
3.The third auscultation point - 2nd left intercostal space close to the sternum. This point is very close to the projection of the pulmonic valve (attachment of upper edge of the III costal cartilage to the sternum). Pulmonary artery valve is listened here.
4.The fourth auscultation point - on the sternum near the xiphoid process. The fourth auscultation point is somewhat lower than the projection of the tricuspid valve and is located near the site of processus xifoideusattachment to the sternum - at the lower part of the sternum to the right. 4 point is a tricuspid valve auscultation point.
5.Fifth (extra) auscultation point - 2/3 of the stethoscope should be put in the left 3rd intercostal space close to the sternum, and 1/3 - on the sternum. This is so-called Botkin-Erb's point1. Aortic valve is listened here.
Currently, auscultation of the heart only in the 5 fixed auscultation points is considered insufficient. According to M.M. Mirrahimov et al. (1981), «the selection of these points is useful when teaching students at the beginning, because it «ties» to each other regions of valve localization and the most frequent place of its auscultation on the anterior chest wall. But for the physician the heart auscultation in the standard points is insufficient due to the fact that the murmurs usually (with rare exceptions) do not cover the point, but the region. At this auscultation point the murmur can only be heard or conducted, and its maximum can be placed between the points. Meanwhile, in the majority of cases, it is possible to assess the murmur properly only in the region of its maximum sounding. This implies that one needs to listen to the entire area of the heart».
30