Материал: Internal_diseases_propedeutics._Part_II._Diagnostics_of_cardiovascular_diseases
In functional or relative mitral incompetence mitral valve is not changed but its ostium is enlarged and valve leaflets close it incompletely. Relative incompetence may develop owing to left ventricle dilatation in myocarditis, myocardidystrophy, myocardiosclerosis, when circular muscle fibers, forming muscle ring around the atrioventricular ostium weaken, and also in papillary muscles damage.
Hemodynamics abnormalities
Hemodynamics in mitral incompetence is characterized by partial blood regurgitation into the left atrium in incomplete closure of mitral valve leaflets. The atrium filling increases since the regurgitated part of blood adds to usual blood volume, arrived from pulmonary veins. Pressure in the left atrium increases, it dilates and hypertrophies.
During diastole greater than normal blood volume flows from overfilled left atrium into the left ventricle, that leads to left ventricle overfilling and dilatation. Left ventricle should work with overload, due to which its hypertrophy develops. Overwork of hypertrophied left atrium and left ventricle protractedly compensates possessed mitral incompetence (Application Fig. 1-3).
In decrease of hypertrophied left atrium contractile capacity congestive phenomena in lesser circulation circle appear and pressure rises, that demands overwork of right ventricle.
So in time in mitral incompetence the right ventricle hypertrophy may develop.
On the heart percussion its dullness enlargement to the left and upwards due to left atrium and left ventricle dilatation is revealed. The heart acquires mitral configuration with smoothed cardiac waist. On right ventricle hypertrophy cardiac dullness also shifts to the right (Fig. 8,9).
21
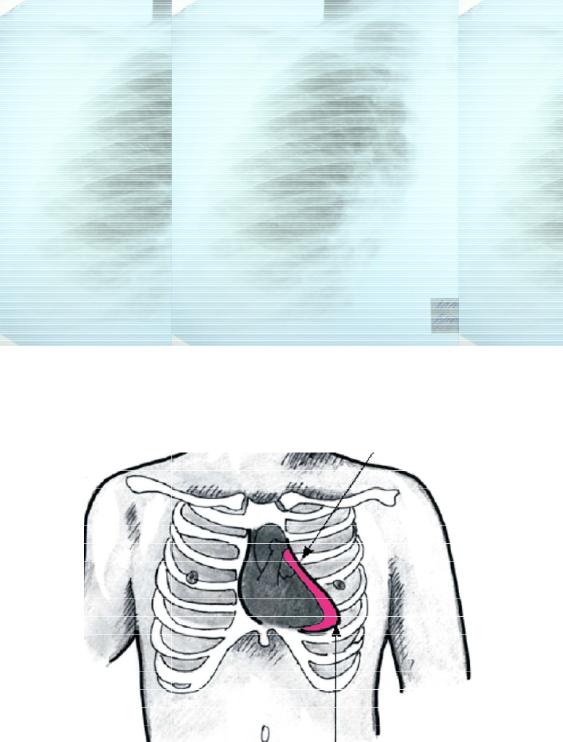
Fig.8. Radiography of t he chest in combined heart defect shows mitral configuration of the heart.
Fig.9. Mitral configuration II of the hea rt.
Aortic heart configur ation – the reasons of this configurati on are stenosis of aortic ostium and aortic incompetence, arterial hypertension.
22
Stenosis of aortic ostium (aortic stenosis, stenosis ostii aortae) creates difficulty for blood ejection into aorta on the left ventricle contraction. Acquired aortic valve stenosis often results from progressive degeneration and calcification of a congenitally bicuspid valve. Rheumatic fever, bacterial endocarditis and arteriosclerotic degeneration are rarer causes.
This valve disease appears owing to adhesion of valve cusps or fibrous narrowing of aortic orifice.
Hemodynamics abnormalities
A little narrowing of aortic orifice doesn’t cause significant circulation alteration. If the degree of stenosis is high, during systole the left ventricle empties incompletely, as all blood volume has no time to pass across narrow orifice into aorta. On diastole normal blood volume from the left atrium adds to this residual blood portion, that leads to left ventricle overfilling and pressure rising within it. This abnormality of intracardiac hemodynamics is compensated by left ventricle overwork, and causes its hypertrophy (Application Fig.7)
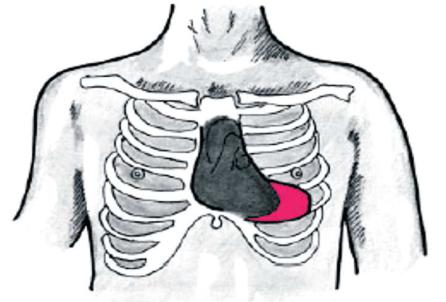
On percussion the displacement of relative dullness borders to the left and aortic heart configuration (with accentuated cardiac waist), caused by left ventricular hypertrophy are detected (Fig.10,11).
Fig.10. Aortic heart configuration.
23
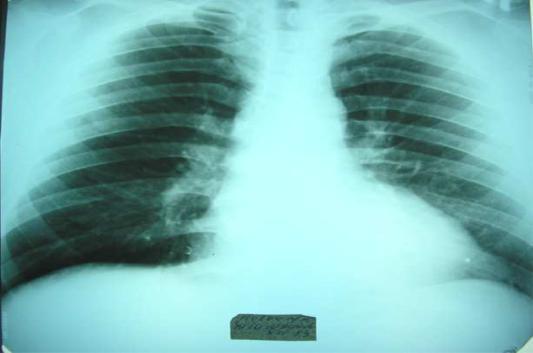
Fig.11. Radiograph y of the chest in aortic incompetence s hows typical aortic configuration of the heart.
Aortic incompetence (i nsufficientia valvulae aortae) is valv e disease in which the semilunar cusps close in completely the aortic orifice and during diastole blood regurgitates from aorta into left ventricle. Aortic regurgitation oc curs if the aortic valve ring dilates, as a result of dissecting aneurysm, ankylosing spondylitis or syphilis for example, or if the valve cu sps degenerate, such as after rheumat ic fever, atherosclerotic lesion or endocarditis.
Anatomical changes d epend on etiology of aortic lesion. After rheumatic fever inflammatory-sclerotic process at the base of valvular cusps lead s to their wrinkling and shortening. In syphilis and a therosclerosis pathologic process may affect only aorta itself, causing its dilatation and taking-up of valvular cusps with out their affecting, or connective tissue expands on valvular cusps and deforms the m. In sepsis ulcerous endocarditis leads to destruction of valve parts, defects forming in the cusps and their subsequent scarring and sho rtening.
Hemodynamics abnor malities
In aortic incompetence during diastole blood comes in the left ventricle not only from left atrium but regurgitates from aorta too. It causes left ventricle overfilling and
24
stretching on diastole. Durin g systole left ventricle contracts with grater force to eject into aorta increased stroke volu me. Left ventricle overwork leads to its hypertrophy, and increase of systolic blood vo lume in aorta causes its dilatation . Sharp fluctuation of blood pressure within aorta during systole and diastole is characteristic for aortic incompetence. Increased as compared with normal blood volume within aorta during systole causes increase of systolic blood pressure, and as a part of blood vo lume regurgitates into ventricle during diastole, dia stolic pressure rapidly decline (Application Fig.5-6).
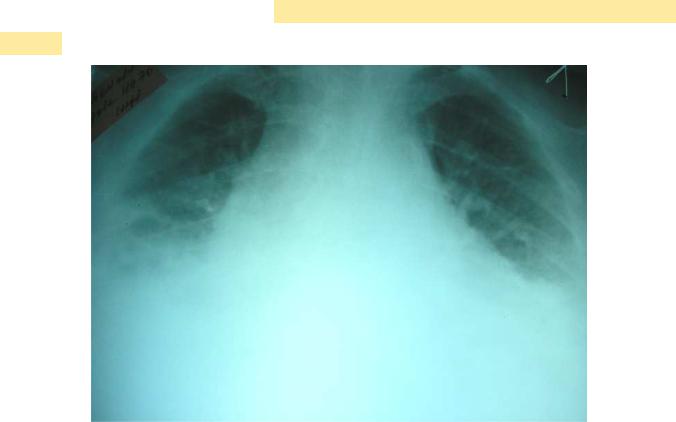
"Trapezoidal" config uration of the heart - the heart has a trapezoid shape, waist of the heart, angle between vena cava superior and right atrium a nd angle between right atrium and diaphragm "di sappear", the reason of configuration is hydropericardium (Fig.12).
Fig.12 "Trapezoidal" configuration of the heart.
" Spherical” configuration of the heart when the ventricular septal defect due to the discharge of blood from the left to the right ventricle.
25