Материал: Internal_diseases_propedeutics._Part_II._Diagnostics_of_cardiovascular_diseases
The properties of the apex beat (left ventricular) (AB): localization (specify intercostal space and the relation to the left midclavicular line), power (weakened, strengthened), square (limited, diffuse), the amplitude (high-amplitude — lift, lowamplitude), resistance, raise or not. In the norm the apex beat is localized in V intercostal space at 1.5 cm medially from the left midclavicular line, at the position on the left side is shifted by 1-1. 5 cm to the left, staying in the V intercostal space.
Fig. 1. Consequence of heart palpation
1. apex beat; 2. cardiac beat; 3. Epigastric pulsation; 4.aorta; 5.pulmonary atery; 6. the jugular fossa
(aorta)
11
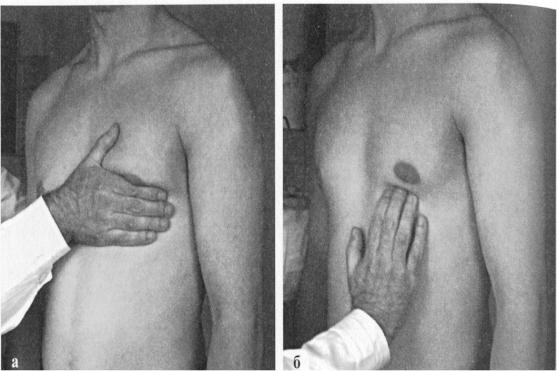
Fig.2 The position of the hands of the doctor at a palpation apex beat.
a. tentative palpation; b. the precise localization, square and power
The reasons for the displacement AB to the left — l eft ventricular hypertrophy
(LVH), right ventricular hypertrophy (RVH), right-sided pneumothorax and hydrothorax, pleuropericardial adhesions and fibrosis on the left.
The reasons for the displacement AB to the right - dextrocardia.
The reasons for the displacement AB up — pregnancy, |
ascites, meteorism, free gas |
in the abdominal cavity. |
|
The reasons for the displacement AB down — viscerop |
tosis, cachexia, post-Natal |
period. |
|
The reasons for the "disappearance" of AB — hydrope ricardium, left-sided hydrothorax.
The reasons for the increase in the area AB (diffuse) - LVH, thin chest, wrinkling the bottom edge of the left lung, enlarged intercostal space and the tumor of the mediastinum.
The reasons for the reduction of the AB (limited) — obesity, swelling of subcutaneous tissue, narrow intercostal space, pulmonary emphysema.
The reasons for increasing the amplitude and strength of the AB — LVH, physical activity, anxiety, thyrotoxicosis.
12
Cardiac (right ventricular)
pathological
epigastric pulsation
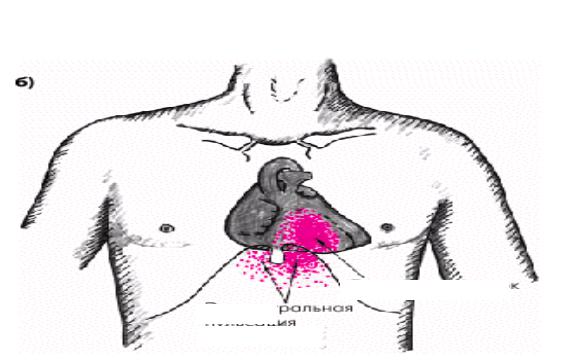
Fig. 3. Cardiac (right ventricular) beat and pathological epigastric pulsation. Cardiac (right ventricular) beat (CB) is a normal palpable as a faint pulsation in the
IV intercostal space at the left edge of the sternum. When hypertrophy and dilatation of the right ventricle shifts CB in the epigastric region, leading to pathological epigastric pulsation (Fig.3).
Thrills in the heart area – is determined by palpat ion. It is necessary to estimate its localization and relation to the phases of cardiac (systolic or diastolic) cycle. Mitral stenosis, for example, leads to diastolic thrill in the apex of the heart. Aortic stenosis leads to a systolic thrill in the II intercostal space to the left of the sternum.
Blood pressure may be measured satisfactorily with a sphygmomanometer of either the aneroid or the mercury type.
Examination of the jugular veins and their pulsations allows quite accurate estimation of the central venous pressure, and therefore gives important information about cardiac compensation.
Plesh test (Plesh J., 1878-1957, Hungarian therapist), syn.: abdominaljugular (or hepato-jugular) reflux. Positive Plesh test occurs in patients with CHF. Palm of the hand for short duration (10 seconds) is pressed against the projection area of the liver in the direction from the bottom upwards. Blood is displaced from the liver into the
13
inferior vena cava and then up to the right atrium, which is manifested by swelling of the neck veins and increase of venous pressure. Pressure on the anterior abdominal wall and an increase in venous blood flow to the heart normally, with adequate contractility of the right ventricle is not accompanied by swelling of the neck veins and increase in central venous pressure (CVP).
In patients with chronic heart failure, with a decrease in the pumping function of the right ventricle and the congestion in the veins of the systemic circulation, abdominaljugular test leads to increased swelling of neck veins and increases CVP at least on 4 cm of water column. Positive abdominal-jugular test indirectly reflects not only the deterioration of hemodynamics of the right heart, but also possible increase in left ventricular filling pressure, i.e. severity of bi-ventricular CHF.
Evaluation of abdominal-jugular test results in most cases helps to clarify the cause of peripheral edema, especially when patients have no significant neck veins extension or other external signs of right ventricular failure. Positive test results indicate the presence of congestion in the veins of the systemic circulation due to the right ventricular failure. Negative result of the test excludes heart failure as the cause of edema. In these cases, one should think of another genesis of edema (hypooncotic edema, shins deep vein thrombophlebitis, calcium antagonists intake, etc.).
Palpation of vessels
Localization of the abdominal aorta pulsation— the lean people, the epigastric region under the xiphoid process, but lower than in prostatic hyperplasia, decreases with a deep breath.
Localization of abnormal aortic arch aneurysm pulsation — the jugular fossa or the handle of the sternum, the so — called retrosternal pulsation.
Localization of abnormal extension of the ascending part of the aorta pulsation - to the right of the sternum in the second intercostal space.
14
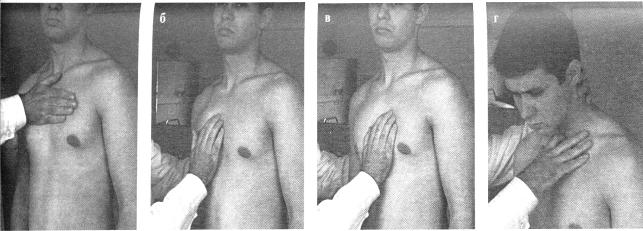
Fig.4. Consequence of vessel palpation.
Examination of arterial pulse. Properties of the pulse at the radial artery (a. radialis). Rate, rhythm, strain, filling, conture, quality of pulse. Equality of pulse on both limbs (Popov-Savelyev's sign).
Examples of changes of the pulse: when aortic stenosis is small, slow, rare; with aortic insufficiency – a large, galloping, frequent .
In case of arrhythmia, specify its type. Pulse deficiency (pulse deficiency is defined [counted] in the presence of atrial fibrillation, at early premature beats).
Arterial pulses can be palpated over the carotid, axillary, brachial, radial, femoral, popliteal, dorsalis pedis, and posterior tibial arteries.
Heart percussion
Main goals of heart percussion are:
1.Disclosure of ventricular and auricular dilation;
2.Disclosure of vascular bundle dilation.
Defining of relative cardiac dullness borders. At first right, left and upper borders of relative cardiac dullness are defined. It is necessary to obtain beforehand an indirect impression about the level of diaphragm standing which influences the results of percussion defining of relative cardiac dullness size. For this purpose the lower border of the right lung is defined along the midclavicular line which is normally located at the level of rib VI.
15