Материал: Internal_diseases_propedeutics._Part_II._Diagnostics_of_cardiovascular_diseases
in significant cusps destruc tion it may not to be heard. In syphi litic and atherosclerotic lesion of aorta S2 may be cl ear enough.
The typical auscultativ e sign of aortic incompetence is diast olic murmur, listened at the aorta and at the BotkinErb's point, which is best heard by sitting the patient upright, leaning forward in full ex piration. It usually is soft, blowing protodiastolic murmur, weakening to the end of diastole as blood pressure decreasing i n aorta and blood flow slowing (Application Fig.4, Fig. 24).
Fig. 24. Diastolic mur mur in aortic regurgitation is located at the 2nd - 4th left interspaces and radiates to the apex, to the right sternal border. The murmur is highpitched, blowing in quality, may be mistaken for breath sounds. I t is heard best with the patient sitting, leaning forwa rd, with breath held in exhalation.
In aortic incompetence at the apex murmurs of functional origin may be also heard. So, in large left ventricular dilatation relative mitral incompeten ce occurs and systolic murmur at the apex appears. Rarely diastolic (presystolic) murmur - Flint's murmur appears due to mitral valve cusps raising by a strong stream of blo od regurgitating during diastole from aorta to left ventricle. It results in difficult blood flow from LA to LV during active atrium systo le. Sometimes in this valve disease two sounds (Traube's doubling sound) and the Vin ogradov-Duroziez‘s doubling murmur heard over the femoral artery are revealed. They are explained by vibration of arterial wal l on systole and diastole during pulse wave passing.
Aortic stenosis: on the heart auscultation at the apex diminished S1, connected with left ventricle overfilling and lengthening of its systole, is listen ed. At the aorta S2 is diminished, in case of adh ered valve cusps immobility it may not be heard. Rough systolic murmur, connected with blood flow across the narrow orifice, at the aorta is
41
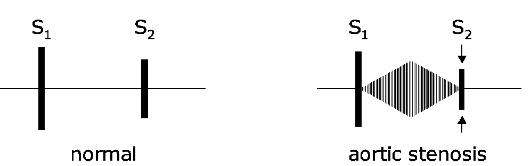
characteristic. It radiates along blood flow direction to the carotids , and sometimes it may be heard at the interscapular area (Application Fig.7, Fig. 25).
Fig. 25. Midsystolic murmur in aortic stenosis is heard in the 2nd right intercostal space, radiates often to the n eck and down the left sternal border, even to the apex. Heard best with the patient sitting a nd leaning forward. A2 decreases as th e stenosis worsens.
Although examination of the alimentary and respiratory sys tems forms part of the complete clinical as sessme nt, palpation of the abdomen for hepat omegaly, firm pressure over the sacrum for dependent oedema, and auscultation over the lung bases are important for the clinical evaluation of the cardiovascular system.
Functional murmurs all the functional murmurs are conditionally divided into three groups:
1.dynamic murmurs, based on significant blood flow velocity increase in absence of any organic cardiac diseases ( for example, dynamic murmurs in thyrotoxicosis, cardiac neurosis, febrile conditions).
2.anemic murmurs, caused by decrease of blood viscosity and certain blood flow acceleration in patients with anemias of different genesis;
3.murmurs of relative valv ular incompetence or relative narrowi ng of valvular openings caused by various valvula r function lesions, including patient s with organic cardiac diseases.
Extracardiac murmur s
Pleuropericardial (ple ural extrapericardial) rub occurs w hen the inflammation process captures part of the pleura, close to the heart, and simu ltaneously the external pericardial layer. This murmur is heard not only in the resp iratory phases, but is synchronic with the heartbeats. To distinguish it from the true pe ricardial rub caused by
42
friction of the inflamed pericardium layers, their attitude to breathing serves. While in true pericarditis friction rub is best heard at breath holding, pleuropericardial rub is best heard at inhalation, sometimes at exhalation, because under these conditions, larger pleural layers surfaces contact with each other (Pletnev D.D., 1928).
Cardiopulmonary murmurs occur in adjacent to the heart parts of the lungs, expanding during systole due to the reduced heart volume. Air penetrating into these parts of the lungs, gives murmur, vesicular in nature («vesicular breath-ing») and systolic in time [«vesicular breathing» with the heart rate] (Chernorutsky M.V., 1954).
Auscultation of vessels
Vinogradov-Durozier's murmur (Vinogradov N.A., 1831-1885, Russian clinician; Durozier Paul Louis, 1826-1897, French physician) is a combination of systolic and diastolic murmurs detected by pressing a stethoscope on the projection area of the femoral artery; it occurs in aortic insufficiency due to reciprocating blood flow through the major arteries.
Murmurs are not heard in a healthy person in ordinary peripheral arteries auscultation. If stethoscope slightly presses on the carotid, subclavian, brachial or femoral arteries, murmur of stenotic origin may appear during their auscultation.
In aortic insufficiency, during auscultation of the femoral artery with a little pressure of stethoscope on it, two murmurs (Vinogradov-Durozier's double murmur) are heard instead of one that can be heard in the normal condition. «First» murmur is caused by artificial narrowing of the arteries, «second» - by the reverse blood flow.
Traube's dual sound (Traube L., 1818-1876, German physician) - auscul-tatory phenomenon: double sound which is heard over the femoral artery. The appearance of Traube's dual sound is a sign of the aortic valve insufficiency.
Two sounds can be heard on auscultation of the carotid and subclavian arteries, one sound is heard on auscultation of the femoral artery, no sound is heard over the brachial artery normally in a healthy person. First sound is quiet, connected with the sudden strain of the arterial wall during admission of blood wave. Second sound (diastolic) is the usual
43
II heart sound, heard on auscultation of the heart and caused by slamming of the aortic valve, but held by the blood flow to the carotid and subclavian arteries.
In case of aortic insufficiency over femoral artery instead of normal one audible sound there two loud sounds are identified, similar to the sound of gun shots (Traube's dual sound).The first sound is caused by the sudden tension of the arterial wall during admission of blood wave, and the second is due to its sudden relaxation because of sharp decrease in blood supply of the femoral artery caused by blood regurgitation into the left ventricle. One should remember, that in aortic insufficiency classic II heart sound disappears and heard over the femoral artery sound is not the II heart sound, held here, but an independent sound, emerging in the femoral artery itself.
It should be kept in mind that both Traube's dual sound, and Vinogradov-Duroziez's dual murmur can be observed not only in aortic insufficiency, but also in infectious diseases, Graves' disease and severe anemia, apparently due to the lowering of the arterial walls tonus (Gubergrits A.J., 1956).
Techniques for improving the auscultation
Sirotinin-Kukoverov's sign (Sirotinin V.N, 1855-1936, Russian therapist; Kukoverov N.G. - assistant doctor of Sirotinin clinic) is appearance (or enhancement in its presence) of systolic murmur at the point of aortic valve auscultation with the patient's raised hands (e.g., at the location of the hands on the hind head). This is the sign of atherosclerotic lesion of ascending thoracic aorta.
Rivero Carvallo sign (Rivero Carvallo J.M.R.) - pathophysiological phenomenon: enhancement of auscultation phenomena (mainly systolic murmur), related to the activities of the right heart, with breath holding during or at the height of a deep inhalation, helps to identify defects of the tricuspid valve. In some guidelines there is error in naming the symptom, it is written incorrectly «Rivero-Carvallo sign». J.M.R. Carvallo was Mexican doctor working at the National Heart Institute in Mexico City. This sign he described in 1946. According to S. Mangione (2004), «medical folklore attributed to him partner (Dr. Rivero), so the sign is often named Rivero-Carvallo sign. In fact, Rivero is one of Carvallo's names.
44

Palpation of the radial pulse
Feeling the right radial pulse has been by tradition the first invasion of a patient's person by his physician. This first contact should therefore transmit warmth, confidence and reassurance. If your hands are cold you should rub them vigorously to warm them. Hold the patient's hand firmly in one hand and feel the pulse with the fingers of the other hand. The first important issue to settle is whether the pulse is present and palpable or absent due to any local or generalized vascular disease.
Next, you need to answer questions about four features of the pulse (Table 5).
The first two of these are comparatively easy and can be answered by counting the pulse rate at least 30 seconds. This is long enough to form an initial opinion about the rhythm, whether regular or irregular due to ectopic beats or completely chaotic as in atrial fibrillation.
|
Table 5. |
|
|
Examination of the pulse |
|
|
|
|
Feature |
Interpretation |
|
|
|
|
Rate |
Resting, 60-80 beats per minute-1 Tachycardia, 90 or more beats per minute- |
|
|
1 Bradycardia, 60 or less beats per minute-1 |
|
|
|
|
Rhythm |
Regular |
|
|
Irregular - ectopic beats or atrial fibrillation Chaotic - atrial fibrillation |
|
|
|
|
Volume |
Normal |
|
|
Large - hypertension, diastolic overload Small - low output states |
|
|
|
|
Character |
Normal |
|
|
Collapsing - aortic incompetence Slow rising - aortic stenosis Bisferiens - |
|
|
aortic stenosis and incompetence |
|
|
|
|
Volume. This is the upstroke of the pulse wave as appreciated by the pulps of the examining fingers, and reflects the pulse pressure or the difference between the systolic and diastolic pressures. It gives some idea about the diastolic burden, output and contractility of the left ventricle. A great deal of experience is required to decide whether
45