Материал: Internal_diseases_propedeutics._Part_II._Diagnostics_of_cardiovascular_diseases
smooth muscle cells, connective tissue, and glycosaminoglycans. Circulating low-density lipoprotein (LDL) migrate through the endothelial barrier of the arterial wall and penetrate into the intima. Some plaques, covered by a thin fibrous cap, may undergo spontaneous fissure or rupture. These plaques are unstable or vulnerable and are more closely associated to the onset of an acute ischemic event.
Ischemic heart disease (IHD; also known as coronary heart disease (CHD) is usually caused by structural disorder of the coronary arteries (coronary artery disease − CAD).
Ischemic heart disease produces six clinical syndromes:
-angina pectoris − stable or unstable, and variant ;
-myocardial infarction (MI);
-postMI cardiosclerosis or old MI;
-heart failure;
-arrhythmias;
-sudden cardiac death.
76
Ischemic heart disease has uncontrollable (advanced age, male sex, genetic predisposition) and modifiable [smoking (risk is almost double), hypertension (risk is double if systolic blood pressure is >180 mm Hg), hyperlipidemia, glucose intolerance or diabetes mellitus, obesity (weight >30% over ideal), hypothyroidism, left ventricular hypertrophy (LVH), sedentary life-style, oral contraceptive use, cocaine use, low serum folates level) risk factors.
Angina pectoris is characterized by discomfort that occurs when myocardial oxygen demand exceeds the supply. Myocardial ischemia can be asymptomatic (silent ischemia), particularly in diabetics.
Pain is located behind the sternum. The usual distribution is referral to all or part of the sternal region, the left side of the chest, and the neck and down the ulnar side of the left forearm and hand.
The most important diagnostic factor is the history.
The physical examination is of little diagnostic help and may be totally normal in many patients.
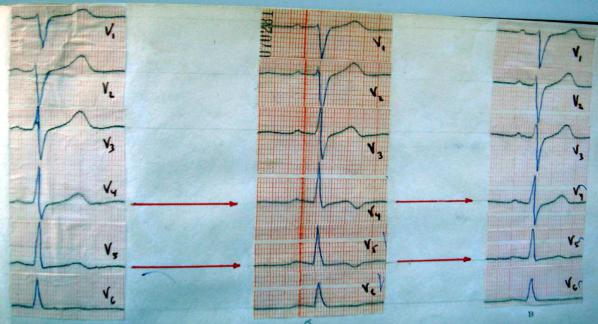
An ECG taken during the acute episode may show transient T-wave inversion or STsegment depression or elevation (may be either convex and concave), but some patients may have a normal tracing.
Fig.27. ECG before, during attack of angina pectoris and after taking nitrates.
77
Ambulatory (Holter) electrocardiographic monitoring can detect silent ischemia (ischemic ECG changes without accompanying symp-toms), which occur in >50% of patients with unstable angina.
Coronary angiography is performed to define the location and extent of coronary disease; this is indicated in selected patients who are candidates for CABG (coronary artery bypass grafting) surgery or angioplasty.
Myocardial infarction (MI) is characterized by necrosis resulting from an insufficient supply of oxygenated blood to an area of the heart.
One distinguishes:
-non−Q wave MI: Area of ischemic necrosis is limit ed to the inner one third to half of myocardial wall;
-Q wave MI: Area of ischemic necrosis penetrates the entire thickness of the ventricular wall. MI may be caused by
• Coronary atherosclerosis
• Coronary artery spasm
• Coronary embolism (caused by infective endocarditis, rheumatic heart disease, intracavitary thrombus)
• Periarteritis and other coronary artery inflammat ory diseases
•Dissection into coronary arteries (aneurysmal or iatrogenic)
•Congenital abnormalities of coronary circulation
•MI with normal coronaries (MINC syndrome): more f requent in younger patients and cocaine addicts.
Echocardiography can evaluate wall motion abnormalities and identify mural thrombus or mitral regurgitation, which can occur acutely after MI.
Clinical presentation of MI:
•Crushing substernal or retrosternal chest pain usually lasts longer than 30 min.
•Pain is unrelieved by rest or sublingual nitroglycerin or is rapidly recurring.
•Pain radiates to the left or right arm, neck, jaw, back, shoulders, or abdomen and is not pleuritic in character.
•Pain may be associated with dyspnea, diaphoresis, nausea, or vomiting.
78
•There is no pain in approximately 20% of infarctions (usually in diabetic or elderly patients).
Physical findings:
Skin may be diaphoretic, with pallor (because of decreased oxygen).
•Rales may be present at the bases of lungs (indic ative of CHF).
•Cardiac auscultation may reveal an apical systoli c murmur caused by mitral regurgitation secondary to papillary muscle dysfunction; S3 or S4 may also be present.
•Physical examination may be completely normal.
•Serum cardiac enzyme studies: damaged necrotic he art muscle releases cardiac isoenzymes (CK, LDH) into the blood stream in amounts that correlate with the size of the infarct. Electrophoretic fractionation of the enzymes can pinpoint certain isoenzymes (CK-MB and LDH-1) that are more sensitive indicators of MI than total CK or LDH. • Cardiac troponin levels: cardiac-specific troponin T (cTnT) and cardiacspecific troponin I (cTnI) are new markers for acute Ml.
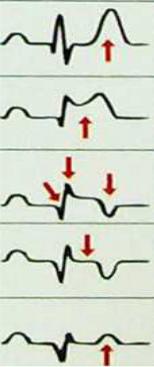
On the ECG in Q wave infarction, there is development of: Common signs
1. (-)T: (ischemia);
2. ST ABOVE CONTOUR, a synonym for "monophasic curve" (damage heart muscle);
3. PATHOLOGICAL Q (necrosis of the heart muscle): the extension Q > 0,03; Q > 1/4R;
4. The DISCORDANCE of the OFFSET ST: ST in leads opposite to the localization of infarction;
5. DYNAMICS (acute phase (injury)-acute-subacute-cicatricial stage). STAGE OF MIOCARDICAL INFARCTION (table 11).
1. Stage of ISCHEMIA;
2. PREACUTE phase (stage of injury): ST above contour;
3. In the ACUTE stage (formation of necrosis): ST above contour with the transition in (-) T; the formation of pathological Q;
79
4.SUBACUTE stage (resorption, proliferation, reparation and organization in the scar area): ST on the contour, T (-), pathological Q;
5.SCAR stage (final consolidation of the scar): ST on the contour, T (-) or (+), pathological Q – in this case, the sign of the scar .
The duration of the stages is subject to the rule of the Troika and the increases on the
rise:
(ISCHEMIA PHASE),
up to 3 days (PREACUTE STAGE),
to 3 weeks (ACUTE PHASE),
to 3 months (SUBACUTE STAGE),
the rest of life (SCAR STAGE).
|
|
|
|
|
Table 11. |
|
|
|
STAGE OF MIOCARDICAL INFARCTION |
||
|
|
|
|
|
|
STAGE |
|
|
DURATION |
|
SIGN |
|
|
|
|
|
|
Stage |
|
of |
|
|
high pointed (coronary) T |
ISCHEMIA |
|
|
to 30 min |
|
wave |
|
|
|
|
|
|
PREACUTE |
|
|
|
|
ST above contour |
phase |
|
|
up to 3 days |
|
|
|
|
|
|
|
|
ACUTE stage |
|
to 3 weeks |
|
ST above contour with the |
|
|
|
|
|
|
transition in (-) T; the |
|
|
|
|
|
formation of pathological Q; |
|
|
|
|
|
|
SUBACUTE |
|
|
|
ST on the contour, T (-), |
|
stage |
|
|
to 3 months |
|
pathological Q; |
|
|
|
|
|
|
SCAR |
stage |
the rest of life |
|
ST on the contour, T (-) or |
|
(final |
|
|
|
|
(+), pathological Q |
consolidation |
of |
|
|
|
|
the scar) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
80 |
|