Материал: npe
Ticket 31
1. Distribution of medicinal substances in the body. Biotransformation of medicinal substances in the body and ways of their excretion. Concept and bioavailability.
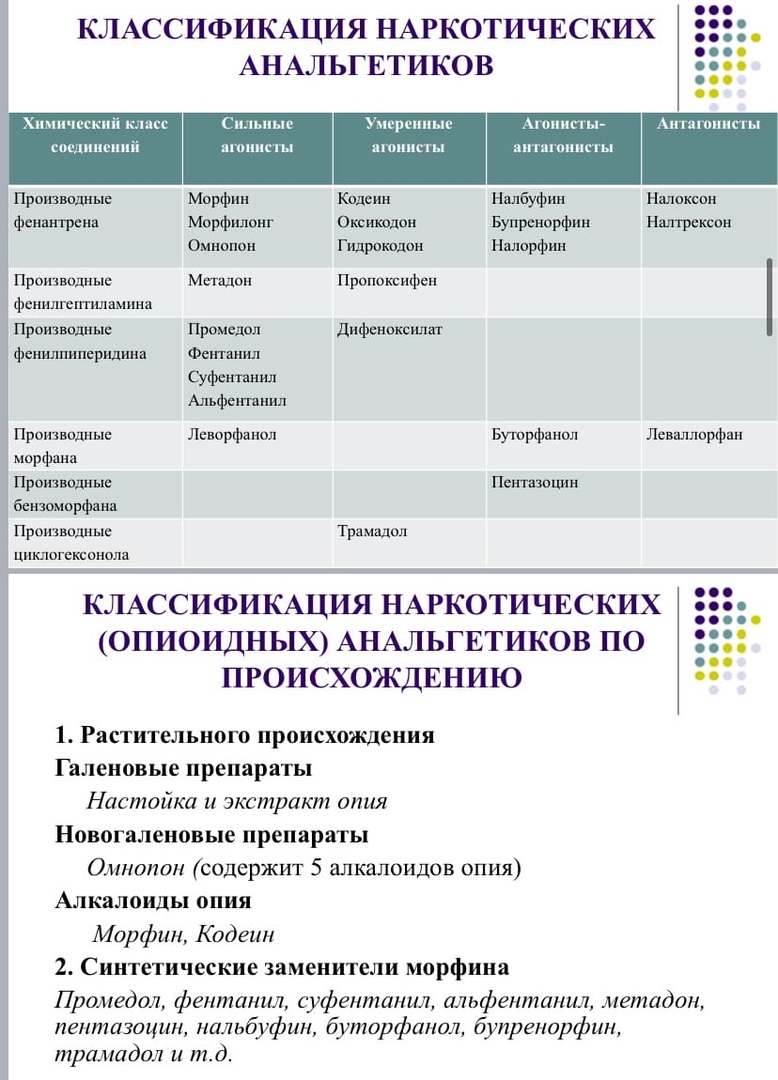
2. Narcotic (opioid) analgesics. Classification. Mechanism of action. Side effects. Contraindications Comparative evaluation of drugs. Antagonists of narcotic analgesics.
3. Laxatives. Classification. Mechanism of action. Indications for use. Side effects. Contraindications Comparative evaluation of drugs.
4. Complications arising from the use of antibiotics, measures for their prevention.
1. Distribution of medicinal substances in the body. Biotransformation of medicinal substances in the body and ways of their excretion. Concept and bioavailability.
1. After absorption, many medicinal substances nonspecifically and reversibly bind to blood plasma proteins, mainly albumin. In this case, different drugs compete with each other for the same binding zones on the surface of the protein and displace each other. Protein-bound drug fractions do not penetrate into tissues and are virtually devoid of pharmacological action. Only the free fraction of the drug in plasma has the ability to penetrate tissues and act. The binding capacity of the blood decreases significantly with protein starvation, liver diseases, extensive burns, with age, and with the replacement of blood loss with protein-free fluids. 2. A dynamic equilibrium is maintained between the free fraction of the drug and the fraction bound by proteins: as the free substance is released into the tissue, its amount is replenished due to the previously bound proteins. When administered intravenously, the following stages occur: - the preparation of the drug in the blood reaches peak concentrations and enters primarily into well-vascularized tissues (heart, brain, kidneys, lungs), which take on the toxic effect; -in the next minutes after administration, the drug is distributed throughout the entire aqueous phase, including organs with slow blood flow (skeletal muscles, subcutaneous tissue) 3. drugs with high lipophilicity are absorbed by adipose tissue, creating a depot that releases the drug as its concentration in the blood decreases brain, kidneys, lungs), which take on the toxic effect; -in the next minutes after administration, the drug is distributed throughout the aqueous phase, including organs with slow blood flow (skeletal muscles, subcutaneous tissue) 3. drugs with high lipophilicity are absorbed by adipose tissue, creating a depot that releases the drug as its concentration in the blood decreases brain, kidneys, lungs), which take on the toxic effect; -in the next minutes after administration, the drug is distributed throughout the entire aqueous phase, including organs with slow blood flow (skeletal muscles, subcutaneous tissue) 3. drugs with high lipophilicity are absorbed by adipose tissue, creating a depot that releases the drug as its concentration in the blood decreases
The significance of biotransformation lies in converting a dangerous substance into a less toxic and water-soluble substance, in order to subsequently remove them with the kidneys, bile, then (excretion routes). This goal is achieved by transferring drug molecules to more polar, more ionized, less lipophilic, less binding to plasma and tissue proteins, less penetrating through biological barriers that are not reabsorbed in the kidneys and intestines.
Biotransformation occurs in the cells of the liver, intestines, lungs, skin and blood plasma. A certain amount is excreted in the urine unchanged.
There are 2 phases of biotransformation: 1) the molecules undergo hydrolysis, oxidation or reduction. 2) When administered orally, the drug begins to undergo biotransformation already in the intestine and during the first passage through the liver, that is, before entering the systemic circulation. This stage of biotransformation is defined as first pass metabolism.
Bioavailability (bioavailability) is characterized by the fraction of the drug from the administered dose that enters the systemic circulation in an active form. Depends on: presystemic metabolism, properties of the drug form, the rate of absorption, conditions affecting the adsorption of drugs.
2. Narcotic (opioid) analgesics. Classification. Mechanism of action. Side effects. Contraindications Comparative evaluation of drugs. Antagonists of narcotic analgesics.
MECHANISMS OF ANALGESIC ACTION OF NARCOTIC ANALGETICS
1. Inhibition of the conduction of pain impulses in the afferent pathways of the central nervous system (impaired transmission of impulses from the endings of the primary afferents to the intercalary neurons of the spinal cord).
2. Strengthening the inhibitory effect of the descending antinociceptive system on the conduction of pain impulses in the afferent pathways of the central nervous system.
3. Change in emotional assessment of pain.
SIDE EFFECTS 1. Nausea, vomiting; 2. Respiratory depression. 3. Bradycardia. 4. Intestinal colic, constipation. 5. Arterial hypotension. 6. With repeated use - addiction, drug dependence. 7. Retention of urination. 8. Increased intracranial pressure.
CONTRAINDICATIONS: 1. Children under 1 year old (morphine - for children under 3 years old). 2. Severe exhaustion. 3. Respiratory failure. 4. Traumatic brain injury (risk of cerebral edema). 5. Paralytic, spastic and obstructive gastrointestinal diseases. 6. Hypertrophy of the prostate gland. 7. Intracranial hypertension. 8. Pregnancy. 9. Fentanyl is contraindicated: during caesarean section (before fetal extraction) and other obstetric manipulations, severe hypertension in the pulmonary circulation, pneumonia, atelectasis, pulmonary infarction, bronchial asthma, parkinsonism (increases muscle stiffness). 10. Butorphanol and pentazocine are not prescribed for patients with coronary artery disease and heart failure.
Comparative characteristics of drugs.
Morphine - acts on the central nervous system, depresses the respiratory center, does not disturb the ventilation of the lungs, depresses the cough center, the vomiting center, stimulates the center of the vagus (bradycardia), increases smooth muscle tone, reduces intestinal secretion and urine output, reduces basal metabolism, causes hyperglycemia, lowers body temperature ...
Promedol is weaker than morphine in terms of analgesic effect, it inhibits the respiratory center less, does not affect uterine contractions during labor, does not spasm smooth muscles, it acts for 3-4 hours.
Fentanyl is 100 times more active than morphine in terms of analgesic effect, inhibits the respiratory center, pain relief after 1-3 minutes for 30 minutes, is used for neuraleptanalgesia.
Codeine - weak analgesic effect, inhibits the cough center, with prolonged use of constipation and dependence.
ANAGONISTS OF NARCOTIC ANALGETICS
Agonist antagonists - nalorphine (blocks μ- and stimulates κ- and δ-receptors)
Antagonists - naloxone, naltrexone (block all types of opioid receptors).
In case of poisoning with narcotic analgesics, respiratory depression is eliminated, all systemic effects of opioid analgesics, including euphoria, are eliminated, causing withdrawal symptoms in drug addicts.
Naloxone lasts for about 1-3 hours, and it must be re-injected, since narcotic analgesics work for a long time. Administered intravenously or intramuscularly. When administered intravenously, it normalizes breathing in 1-2 minutes. In addition, the drug is used for alcoholic coma, shock conditions, and some mental illnesses.
Naltrexone acts like naloxone, but for a longer period - up to 24-40 hours, is used orally, in tablets, the effect occurs after 1-2 hours.
Nalorphine is rarely used in case of an overdose of narcotic analgesics.
3. Laxatives. Classification. Mechanism of action. Indications for use. Side effects. Contraindications Comparative evaluation of drugs.
Classification:
I. Laxatives that inhibit absorption and stimulate secretion. -Inorganic substances Saline laxatives Magnesium sulfate Sodium sulfate --Organic remedies 1. Of plant origin a) Vegetable oils-Castor oil b) Preparations containing anthraglycosides: Buckthorn extract liquid (dry), Rhubarb tablets, Infusion of senna leaves 2. Synthetic means: Phenolphthalein , Izaphenin, Bisacodyl, Guttalax II. Means that increase the volume of intestinal contents: Seaweed, Laminarid, Wheat bran, Lactulose (normase), Forlax, Mucofalk III. Means that lubricate the intestinal mucosa and soften feces :: Vaseline oil, Almond oil IV. Laxative suppositories (gas-generating candles): Ferrolax, Calciolax
Laxatives that inhibit absorption and stimulate secretion. Means to increase the volume of intestinal contents
Means that lubricate the intestinal mucosa and soften stool
Inorganic laxative suppositories organic
Indications: Drugs of this group are used to obtain a strong single laxative effect, for example, for: - acute poisoning; - acute constipation; - before surgery to cleanse the intestines; - before proctological studies; - together with some antihelminthic drugs for expelling worms.
Herbal origin Preparations of this group are used to obtain a strong single laxative effect, for example, for: - acute poisoning; - acute constipation; - before surgery to cleanse the intestines; - before proctological studies; - together with some antihelminthic drugs for expelling worms.
Synthetic drugs Used for chronic constipation of various etiologies caused by hypotension and sluggish peristalsis of the large intestine, incl. in elderly people, in bedridden patients, in the postoperative period, after childbirth; for stool regulation for hemorrhoids, proctitis, anal fissures; cleansing the intestine during preoperative preparation, to prepare the colon for instrumental and X-ray examinations. It is used for chronic constipation, diseases and conditions, the treatment of which should be accompanied by mild defecation (hemorrhoids, anal fissure, pregnancy, postoperative period after surgery on the rectum), diarrhea of various etiologies, irritable bowel syndrome.
Side effects: inhibition of the structures of the brain that regulate respiration and vascular tone, causes relaxation of vascular smooth muscles and leads to a decrease in blood pressure. Magnesium sulfate can cause sedative or hypnotic effects, disrupt neuromuscular transmission or uterine contractile activity. moderate spastic abdominal pain; - malabsorption; - hypokalemia some patients may experience intestinal colic, palpitations and even collapse. There are allergic reactions (up to shock) with repeated use of the medication. possible allergic reactions to the components of the drug, increased gas formation in the intestines in the first days of therapy, feeling of a full intestine. With prolonged use, the prdigestion process.
Contraindications: heart or renal failure; acute poisoning with fat-soluble poisons (kerosene, gasoline). Intestinal obstruction, acute inflammation of the gastrointestinal tract, strangulated hernia, intestinal bleeding, Acute proctitis, acute hemorrhoids, intestinal obstruction, strangulated hernia, peritonitis, acute gastrointestinal diseases, uterine bleeding, cystitis.
Mechanism: Gastrointestinal drugs dissociate to form ions that are poorly absorbed. This leads to an increase in osmotic pressure in the intestinal lumen, which prevents the absorption of the liquid part of the chyme and digestive juices. The volume of intestinal contents increases, this leads to irritation of mechanoreceptors and increased peristalsis. Saline laxatives act mainly in the small intestine. The effect occurs in 4 - 6 hours from the moment of administration.
In the duodenum, under the action of pancreatic lipase, castor oil is hydrolyzed with the release of glycerol and ricinolic acid, the latter irritates the cells of the intestinal mucosa, inhibits the process of active absorption of water and electrolytes, which leads to increased motility and accelerates bowel emptying, and glycerin, obstruction - kinky mucous membrane, facilitates the movement of contents. The effect appears after 2-6 hours
The mechanism of action consists in inhibition of Na + -K + -ATPase of the intestinal mucosa membranes (absorption of sodium and water is impaired) and in influencing the effects of calcium in intestinal smooth muscle cells. The drugs of this group are not absorbed in the gastrointestinal tract, they adsorb water on their surface, swell, thereby increasing the volume of the indigestible residue. Thus, they represent a mechanical stimulus, since they cause stretching of ki.the intestine and increase its motor skills. When taken orally, the feces are not absorbed and soften.