Материал: Atrial Fibrillation- Management
Atrial Fibrillation – Management
Brian Olshansky, MD
Warfarin – therapeutic range
•INR 2.0 - 3.0 = therapeutic range
•INR > 2 = risk of bleeding ↑, no reduction in risk for stroke
•INR < 2 = risk of stroke ↑↑
 Hylek EM. N Engl J Med 1996; 335:540–546
Hylek EM. N Engl J Med 1996; 335:540–546
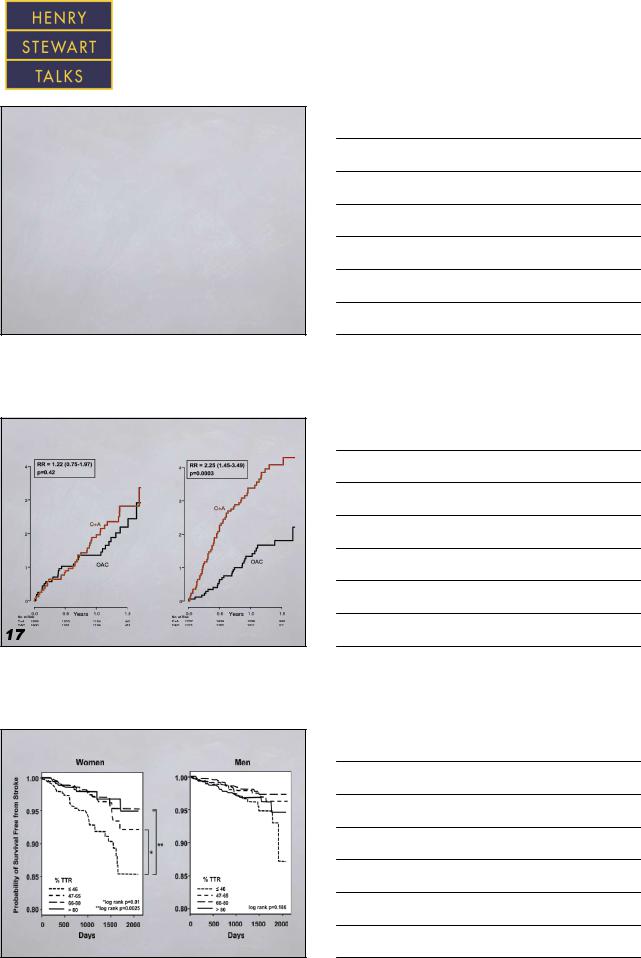
Time in therapeutic range (TTR)
TTR<65% TTR≥65%
Thromboembolism % |
Thromboembolism % |
C+A = clopidogrel and aspirin
OAC = oral anticoagulation
Connolly S. Circulation. 2008; 118:2029-2037
AFFIRM - gender differences
 Sullivan RM. Am Heart J 2012 in press
Sullivan RM. Am Heart J 2012 in press
The screen versions of these slides have full details of copyright and acknowledgements |
6 |
Atrial Fibrillation – Management
Brian Olshansky, MD
HAS-BLED bleeding risk score
Letter |
|
Clinical characteristic |
|
Points awarded |
|
|
|||
H |
|
Hypertension |
|
1 |
A |
|
Abnormal renal |
|
1 or 2 |
|
and liver function |
|
||
S |
|
Stroke |
|
1 |
B |
|
Bleeding |
|
1 |
L |
|
Labile INRs |
|
1 |
E |
|
Elderly (i.e., age >65 years) |
|
1 |
D |
|
Drugs or alcohol |
|
1 or 2 |
|
(1 point each) |
|
||
|
|
|
|
|
|
|
|
|
Maximum 9 points |
Pisters R. Chest 2010; 138:1093-1100 |
|
|
||
CammAJ. Eur Heart J 2010; 31:2369-2429 |
|
|
||
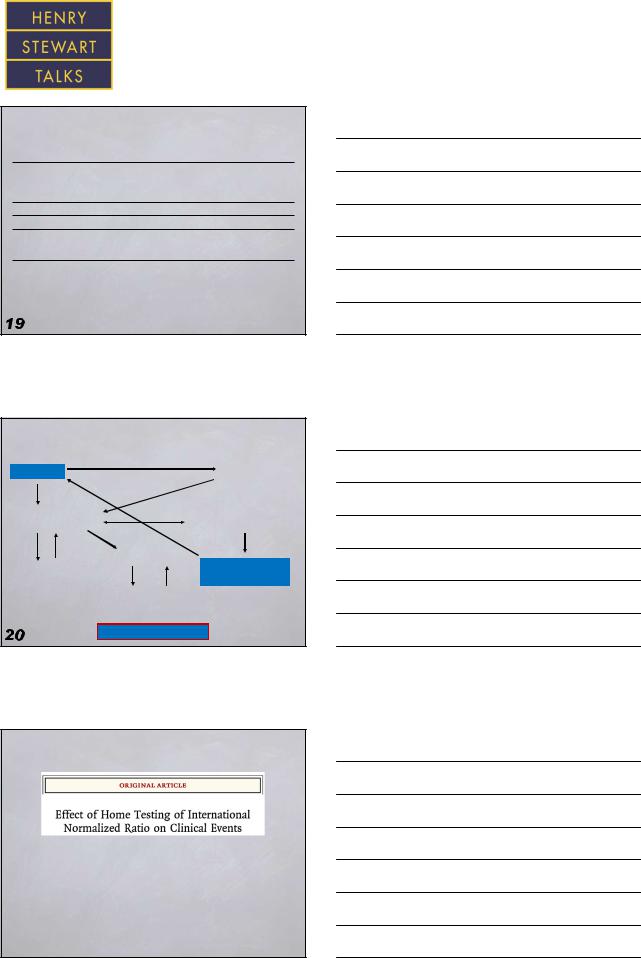
Traditional anticoagulation
Office visit |
Warfarin |
Send patient |
|
to lab for PT/INR |
|
Report data |
|
Patient contacted for |
by fax, phone |
dosage change, if needed |
|
Patient chart pulled |
|
Repeat sequence |
Nurse reviews data |
Data entered on chart |
every 1-8 weeks |
Warfarin is no one’s favorite drug
Is there a better way?
Is home monitoring the answer?
First event with home monitoring the same as clinic testing
 Matchar DB. N Engl J Med 2010; 363:1608-20
Matchar DB. N Engl J Med 2010; 363:1608-20
The screen versions of these slides have full details of copyright and acknowledgements |
7 |
Atrial Fibrillation – Management
Brian Olshansky, MD
Other anticoagulants
•Aspirin
•Clopidogrel (and in combination)
•Direct thrombin inhibitors (dabigatran)
•Direct factor Xa inhibitors
(rivaroxaban, apixaban, betrixaban, edoxaban)
ACTIVE trial
Clopidogrel plus aspirin combination was slightly better than aspirin alone
 Connolly S. N Engl J Med 2009; 360:2066-78
Connolly S. N Engl J Med 2009; 360:2066-78
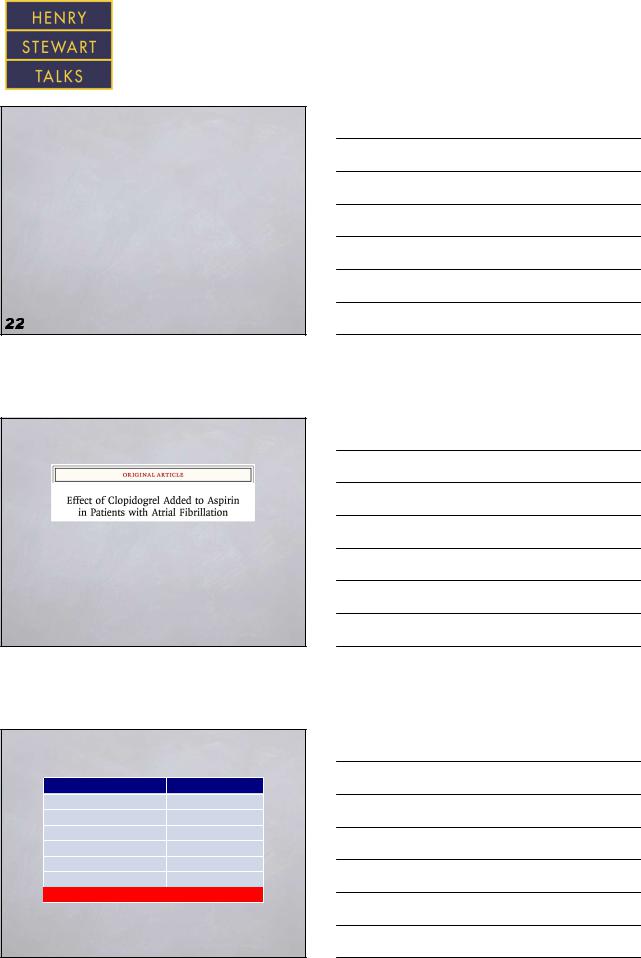
Anticoagulation for AF and bleeding
Therapy |
HR (95% CI) |
Warfarin monotherapy |
1 [reference] |
Aspirin monotherapy |
0.93 (0.88-0.98) |
Clopidogrel monotherapy |
1.06 (0.87-1.29) |
Aspirin + clopidogrel |
1.66 (1.34-2.04) |
Warfarin + aspirin |
1.83 (1.72-1.96) |
Warfarin + clopidogrel |
3.08 (2.32-3.91) |
Triple therapy |
3.70 (2.89-4.76) |
 Hansen ML. Arch Intern Med 2010; 170:1433-1441
Hansen ML. Arch Intern Med 2010; 170:1433-1441
The screen versions of these slides have full details of copyright and acknowledgements |
8 |
Atrial Fibrillation – Management
Brian Olshansky, MD
RE-LY: dabigatran
Connolly SJ. N Engl J Med 2009; 361:1139-1151
Mean CHADS2 – 2.1; TTR 64%
•Dabigatran 150 mg twice a day was associated with a lower risk for stroke and thromboembolism, compared to warfarin or 110 mg bid dose
•Dabigatran does not require measurements of an INR, it may be superior to warfarin
•Hard to determine the level of anticoagulation
•Risk of bleeding
•Expanse
ROCKET AF: rivaroxaban
Patel MR. N Engl J Med 2011; 365:883-891
•Rivaroxaban: 20 mg daily
•TTR 55%
•CHADS2 – 3.5
•There was no significant difference in the event rate over time (warfarin vs. rivaroxaban)
AVERROES: apixaban
Apixaban was superior to aspirin in terms of number of strokes or systemic embolic events in the long term follow up
Connolly S. N Engl J Med 2011; 364:806-17
The screen versions of these slides have full details of copyright and acknowledgements |
9 |
Atrial Fibrillation – Management
Brian Olshansky, MD
ARISTOTLE: apixaban
Granger CB. N Engl J Med 2011; 365:981-992
•Apixaban was superior in terms of the rate
of thromboembolic events, major bleeding events
•CHADS2 – 2.1
•Apixaban 5 mg bid
•TTR 62%
ACC/AHA guidelines
|
Risk category |
|
Recommendation |
|
|
|
|
||
|
|
|
Oral anticoagulantion recommended |
|
|
With prior stroke, TIA, |
|
(Warfarin IA, dabigatran, rivaroxaban, |
|
|
|
or apixaban IB) |
|
|
|
or CHA2DS2-VASc |
|
Direct thrombin or factor Xa inhibitor |
|
|
score ≥2 |
|
|
|
|
|
recommended if unable to maintain |
|
|
|
|
|
therapeutic INR I C |
|
|
With nonvalvular AF |
|
Reasonable to omit antithrombotic therapy |
|
|
and CHA2DS2-VASc |
|
|
|
|
score of 0 |
|
|
|
|
With nonvalvular AF |
|
No antithrombotic therapy or treatment |
|
|
and a CHA2DS2-VASc |
|
with oral anticoagulant or aspirin |
|
|
score of 1 |
|
may be considered |
|
 Fuster V. Circulation 2006; 114:e257-e354
Fuster V. Circulation 2006; 114:e257-e354
Anticoagulation – the bottom line
•Warfarin – gold standard, “high risk” patients
–Despite the fact that clinical trials show benefits of novel anticoagulants:
1.Long term experience
2.We can measure the level of anticoagulation
3.Less expensive
4.Renal/valvular heart disease issues
•“Risk” is still being refined
•Dabigatran or another drug may replace warfarin soon (even in lower risk patients)
The screen versions of these slides have full details of copyright and acknowledgements |
10 |