Материал: Atrial Fibrillation- Management
Atrial Fibrillation – Management
Brian Olshansky, MD
Atrial Fibrillation – Management
The Challenge and New Solutions
(Part 1 of 2)
Brian Olshansky, MD
Professor Emeritus of Medicine
University of Iowa Hospitals
72 yo female with palpitations
•CC: debilitating fatigue, dyspnea 2-3 times/day
•PMH: hypertension, diabetes
•Meds: metoprolol 25 mg bid
•Px: BP: 144/94, P: 120, irregular
–Lungs: clear
–Heart: normal S1 and S2
Electrocardiogram
The screen versions of these slides have full details of copyright and acknowledgements |
1 |
Atrial Fibrillation – Management
Brian Olshansky, MD
Echocardiogram
•Normal left ventricular function
•No valvular abnormalities
•LV wall thickness = 1.3 cm
•LA size = 4.2 cm
Event monitor
•Episodes of sinus rhythm
•Episodes of asymptomatic atrial fibrillation
•Episodes of rapid rates in atrial fibrillation during symptoms
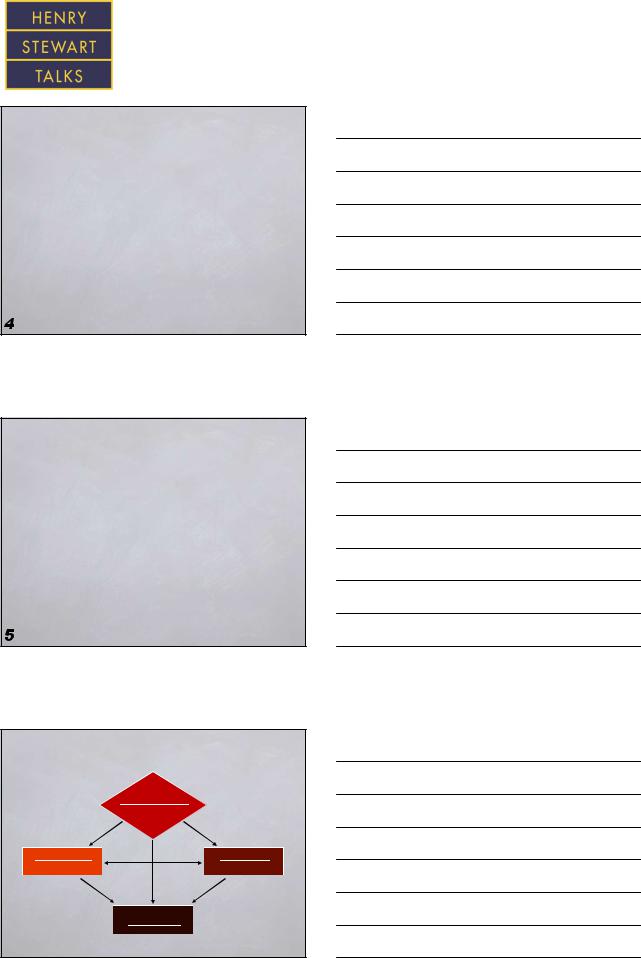
Atrial fibrillation - classification
|
New/recurrent |
|
≥2 episodes |
Paroxysmal |
Persistent |
≤7 days |
>7 days |
Permanent
 Fuster V. Circulation 2006; 114:e257-e354
Fuster V. Circulation 2006; 114:e257-e354
The screen versions of these slides have full details of copyright and acknowledgements |
2 |
Atrial Fibrillation – Management
Brian Olshansky, MD
Why treat atrial fibrillation?
•Eliminate symptoms
•Reduce risk of stroke
•Reduce risk of heart failure
•Improve survival (?)
•Eliminate atrial fibrillation (?)
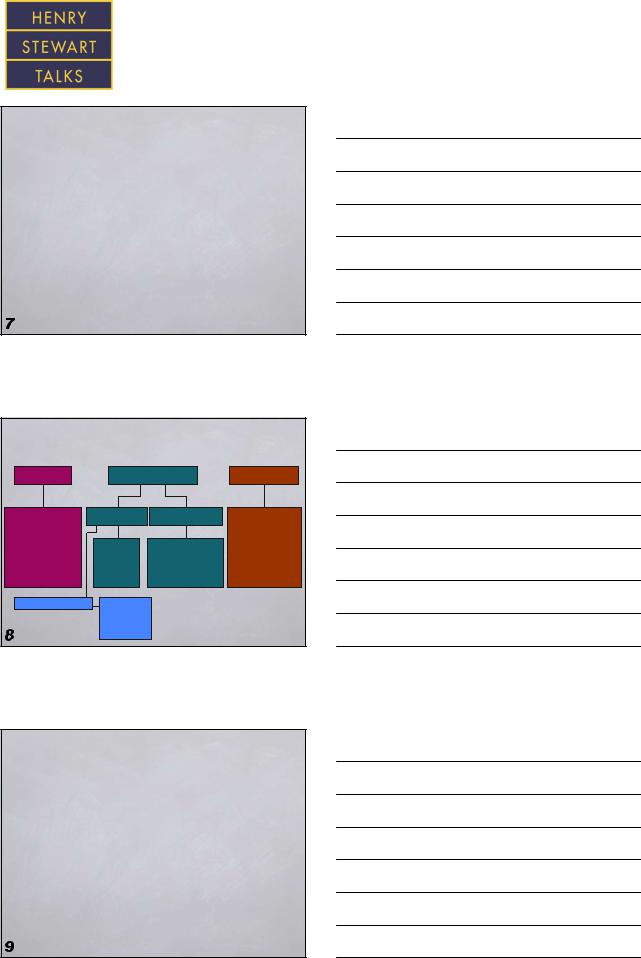
Treatment goals and strategies
|
Rate control |
Maintenance of SR |
Stroke prevention |
|
Pharmacologic |
Pharmacologic |
Nonpharmacologic |
Pharmacologic |
|
• |
Ca2+ blockers |
|
|
• Warfarin |
• |
β-blockers |
• Class IA |
• Catheter ablation |
• Aspirin |
• |
Digitalis |
• Thrombin Inhibitor |
||
• |
Amiodarone |
• Class IC |
• Pacing |
Nonpharmacologic |
Nonpharmacologic |
• Class III |
• Surgery |
• Removal/isolation |
|
• |
Ablate and pace |
• β-blocker |
• Implantable devices |
LA appendage |
|
Prevent remodeling |
• CCB |
|
|
|
|
• ACE-I, ARB |
|
|
• Statins
• Fish oil
Approach to treatment
Any (or all) may apply
•Anticoagulation
•Ventricular rate control
•Maintenance of sinus rhythm
The screen versions of these slides have full details of copyright and acknowledgements |
3 |
Atrial Fibrillation – Management
Brian Olshansky, MD
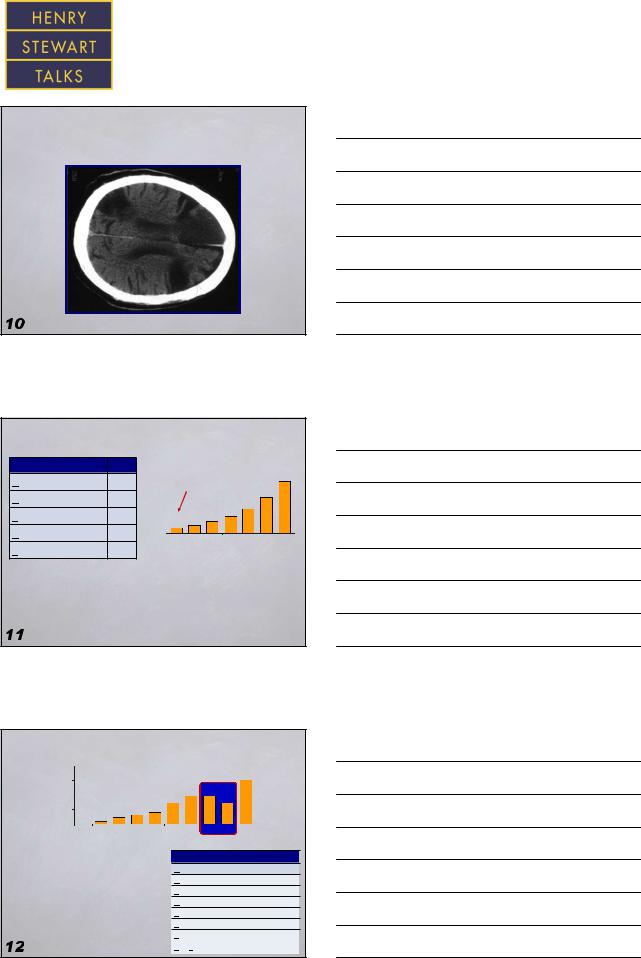
Patient with AF not anticoagulated
Complaint - dizziness
CHADS2 risk stratification
Risk factor |
Score |
Congestive heart failure |
1 |
HTN |
1 |
Age ≥75 y |
1 |
Diabetes |
1 |
Stroke |
2 |
Stroke rate, %
20 |
|
|
|
|
|
|
18.2 |
15 |
|
|
|
|
8.5 |
12.5 |
|
10 |
|
2.8 |
4.0 |
5.9 |
|
|
|
5 |
1.9 |
|
|
|
|||
0 |
0 |
1 |
2 |
3 |
4 |
5 |
6 |
|
|
|
CHADS2 score |
|
|
||
CHA2DS2-VASc now recommended
Rietbrock S. Am Heart J 2008; 156:57-64
Chugh SS. J Am Coll Cardiol 2001; 37:371-78
Rockson SG. J Am Coll Cardiol 2004; 43:929-935
CHA2S2-VASc risk stratification
% |
20 |
|
|
|
|
|
|
|
|
|
|
|
15.2 |
|
|
15 |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
rate, |
|
|
|
|
|
|
|
|
9.8 |
9.6 |
|
|
|
|
|
10 |
|
|
|
|
|
|
6.7 |
6.7 |
|
|
|
||||
Stroke |
5 |
0 |
1.3 |
2.2 |
|
3.2 |
4.0 |
|
|
|
|
|
|
|
|
|
0 |
0 |
1 |
2 |
|
3 |
4 |
5 |
6 |
7 |
8 |
9 |
|
|
|
|
|
|
|
|
CHA2DS2-VAScscore |
|
|
|
|
|
|||||
• The CHA2DS2-VASc score |
|
|
|
Risk factor |
|
|
Score |
|
|||||||
|
|
|
|
|
|
||||||||||
|
|
|
Congestive heart failure |
1 |
|
||||||||||
and bleeding risk score overlap |
|
|
HTN |
|
|
|
1 |
|
|||||||
• Who should or should not |
|
|
|
|
Age ≥75 y |
|
|
2 |
|
||||||
get anticoagulants |
|
|
|
|
|
|
Diabetes |
|
|
|
1 |
|
|||
|
|
|
|
|
|
Stroke |
|
|
|
2 |
|
||||
– e.g. frailty in old age population |
|
|
Vascular disease |
|
1 |
|
|||||||||
(cost>benefit) |
|
|
|
|
|
|
Age 65-74 y |
|
|
1 |
|
||||
Lip GYH. Am J Med 2010; 123:484-488 |
|
|
|
Sex category (female) |
1 |
|
|||||||||
The screen versions of these slides have full details of copyright and acknowledgements |
4 |
Atrial Fibrillation – Management
Brian Olshansky, MD
ASSERT trial
Subclinical atrial tachycardias and stroke
•Atrial tachycardia > 6 minutes, rate >190 bpm → greater risk for stroke
•2580 patients with pacemaker or ICDs
•Patients in the ASSERT trial with CHADS2 score of 1 with 1 event/year of AT/AF have 0.56 %/year – not enough for aggressive anticoagulation
 Healy J. New Engl J Med 2012; 366:120-129
Healy J. New Engl J Med 2012; 366:120-129
Warfarin
•The gold standard
•No one’s favorite drug
•Requires time in therapeutic range
•Gender differences exist
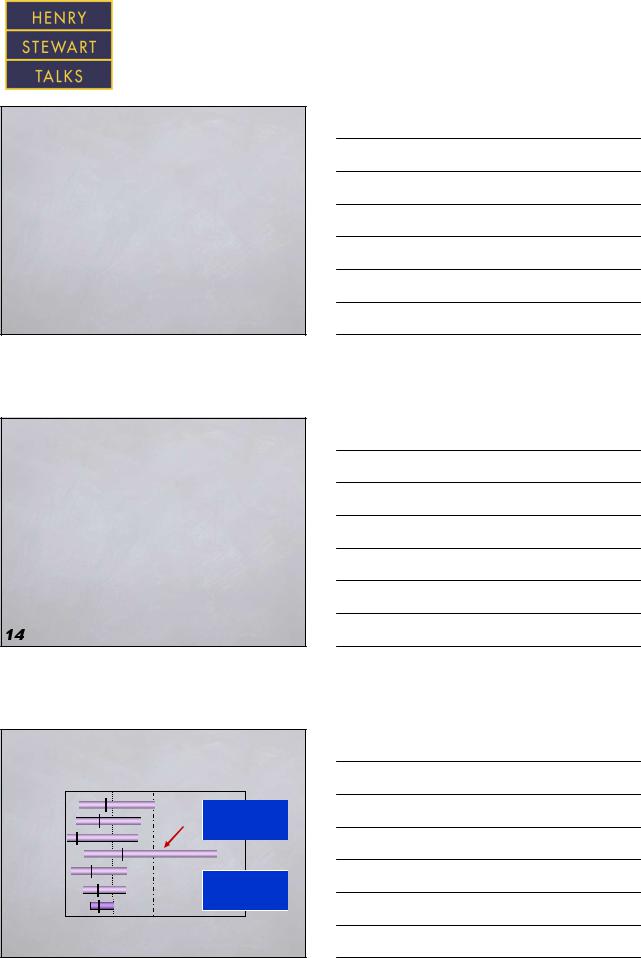
Warfarin anticoagulation in AF
|
Warfarin better |
|
Control better |
|
AFASAK |
|
|
|
Reduction of |
SPAF |
|
|
|
all-cause mortality |
BAATAF |
|
|
|
RRR 26% |
CAFA |
|
|
|
|
SPINAF |
|
|
|
Reduction |
EAFT |
|
|
|
of stroke |
Aggregate |
|
|
|
RRR 62% |
100% |
50% |
0 |
-50% |
-100% |
 Hart RG. Ann Intern Med 1999; 131:492-501
Hart RG. Ann Intern Med 1999; 131:492-501
The screen versions of these slides have full details of copyright and acknowledgements |
5 |