Материал: part20
DICOM PS3.20 2020a - Imaging Reports using HL7 Clinical Document Architecture |
Page 121 |
C SR to CDA Imaging Report Transformation
Guide
Constrained DICOM SR documents based on Imaging Report templates can be mapped to HL7 CDA Release 2 Imaging Reports basedonTemplate1.2.840.10008.9.1,asspecifiedinSection7.1.TheSRreporttemplatestowhichthistransformationappliesinclude:
•TID 2000 Basic Diagnostic Imaging Report
•TID 2005 Transcribed Diagnostic Imaging Report
•TID 2006 Imaging Report With Conditional Radiation Exposure and Protection Information
SR instances based on other templates may also be able to be mapped using the transformations in this Annex.
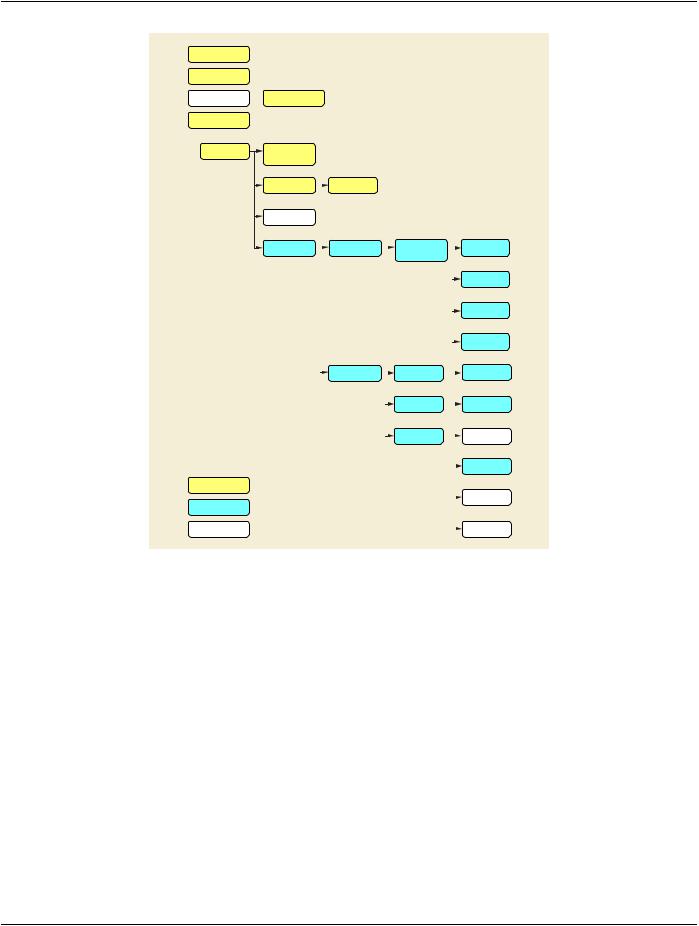
SR documents can be thought of as consisting of a document header and a document body, corresponding to a CDA document header and body. The header includes the modules related to the Patient, Study, Series, and Equipment Information Entities, plus the SR Document General Module, as specified in PS3.3. The SR Document Content Module contains the content tree (structured content) of the document body. Note, however, that DICOM SR considers the root content item, including the coded report title, and somecontext-settingcontentitemsaspartofthedocumentbodycontenttree,buttheseconstitutepartoftheCDAheader.SeeFigureC- 1.
C.1 Constraints
This Annex defines the transformation of an Enhanced SR SOP Instance to a CDA instance. The following constraints apply to such SOP Instances:
•Observation Context: The mapping does not support changing the observation context for the report as a whole from its default context, as specified in the Patient, Study, and Document Information Entities (see PS3.3 Section C.17.5 “Observation Context Encoding”)
Note
TID 2000, TID 2005 and TID 2006 specify inclusion of TID 1001 Observation Context as Mandatory, but TID 1001 has no content if all aspects of context are inherited, as under this constraint.
•Subject Context: The mapping does not support the subject of any of the report sections to be a specimen TID 1009), a device (TID 1010), or a non-human subject. Only a fetus subject context is supported for a Findings section.
•Procedure Context: The mapping allows identification of a different procedure than the procedure identified in the SR Study IE only as context for a Prior Procedure Descriptions section.
•De-identified Documents: There is no CDA implementation guidance from HL7 for de-identified documents, other than general rules for using the MSK null flavor (see Section 5.3.2). There is no CDA capability equivalent to the Encrypted Attributes Sequence (see PS3.3 Section C.12.1.1.4.1 “Encrypted Attributes Sequence”) for carrying encrypted re-identification data.
•Patient Study Module: Medical or clinical characteristics of the patient specified in the Patient Study Module are not mapped (see PS3.3 Section C.17.5 “Observation Context Encoding”)
•Clinical Trials: Template 1.2.840.10008.9.1 does not define attributes for clinical trials equivalent to those of the Patient, Study, and Series IEs (Clinical Trial Subject Module, Clinical Trial Study Module, Clinical Trial Series Module).
•Spatial Coordinates: The mapping does not support SCOORD observations. As CDA documents are principally for human reading, detailed ROI data is presumed to reside in the DICOM SOP Instances of the study, or in images ready for rendering with a Presentation State, not in the CDA report. Template 1.2.840.10008.9.1 does not support the CDA Region of Interest Overlay entry class (see Section 9.1.2.4).
- Standard -
Page 122 |
DICOM PS3.20 2020a - Imaging Reports using HL7 Clinical Document Architecture |
Patient IE
Study IE
Series IE
Document IE
Document General Module
TID 2000
Basic Diagnostic
Imaging Report
Mapped to CDA Header
Mapped to CDA Body
Not supported in Mapping
Equipment IE
TID 1204
Language of
Content Item and
Descendants
TID 1210 |
|
TID 1201 |
|
|
|
|
|
|
|
||
Equivalent Meaning(s) |
|
|
Language of Value |
|
|
|
|
|
|
|
|
of Concept Name |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
||
TID 1001 |
|
|
|
|
|
|
|
|
|
|
|
Observer Context |
|
|
|
|
|
|
|
|
|
|
|
CONTAINER |
|
TID 2002 |
|
|
TID 2001 |
|
|
TID 1400 |
|||
(heading) |
|
|
Report Narrative |
|
|
Basic Diagnostic |
|
|
Linear |
||
|
|
|
|
|
|
|
Imaging Report |
|
|
Measurements |
|
|
|
|
|
|
|
|
Observations |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TID 1401 |
|
|
|
|
|
|
|
|
|
|
|
Area |
|
|
|
|
|
|
|
|
|
|
|
Measurements |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TID 1402 |
|
|
|
|
|
|
|
|
|
|
|
Volume |
|
|
|
|
|
|
|
|
|
|
|
Measurements |
|
|
|
|
|
|
|
|
|
|
|
TID 1404 |
|
|
|
|
|
|
|
|
|
|
|
Numeric |
|
|
|
TID 1001 |
|
|
TID 1002 |
|
|
Measurements |
||
|
|
|
|
|
|
|
TID 1003 |
||||
|
|
|
Observer Context |
|
|
|
Observer Context |
|
|
|
Person Observer |
|
|
|
|
|
|
|
|
|
Identifying Attributes |
||
|
|
|
|
|
|
|
TID 1005 |
|
|
TID 1004 |
|
|
|
|
|
|
|
|
Procedure Context |
|
|
Device Observer |
|
|
|
|
|
|
|
|
|
|
Identifying Attributes |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TID 1006 |
|
|
TID 1007 |
|
|
|
|
|
|
|
|
Subject Context |
|
|
|
Subject Context, |
|
|
|
|
|
|
|
|
|
|
|
Patient |
|
|
|
|
|
|
|
|
|
|
|
TID 1008 |
|
|
|
|
|
|
|
|
|
|
|
Subject Context, |
|
|
|
|
|
|
|
|
|
|
|
Fetus |
|
|
|
|
|
|
|
|
|
|
|
TID 1009 |
|
|
|
|
|
|
|
|
|
|
|
Subject Context, |
|
|
|
|
|
|
|
|
|
|
|
Specimen |
|
|
|
|
|
|
|
|
|
|
|
TID 1010 |
|
|
|
|
|
|
|
|
|
|
|
Subject Context, |
|
|
|
|
|
|
|
|
|
|
|
Device |
Figure C-1. TID 2000 Structure Summarized from PS3.16, and mapping to CDA
C.2 Conventions
Literal values to be encoded in CDA elements are represented in the mapping tables in normal font, as a string, or as a coded value triplet:
"NI"
(codeValue, codingScheme, codeMeaning)
Conventions for mapping from DICOM attributes in the transformed SR are described in Section 5.2.8.
Data mapped from an SR Content Item is identified by the Concept Name of the Content Item, represented in the mapping tables as a triplet in italic font:
(codeValue, codingScheme, codeMeaning)
Data mapped from a specific Attribute in an SR Content Item uses the triplet to identify the Content Item, with the > character and the specific attribute name and tag:
(codeValue, codingScheme, codeMeaning) > Attribute Name (gggg,eeee)
- Standard -
DICOM PS3.20 2020a - Imaging Reports using HL7 Clinical Document Architecture |
Page 123 |
Additional notes are within square brackets:
[Note]
Mandatory CDA elements for which there is no corresponding source data in the SR SOP Instance may be coded with a nullFlavor attribute (see Section 5.3.2).
C.3 Header Transformation
For transformation of the SR content into the CDA header, the target elements of the CDA instance are listed in Table C.3-1 by their Business Names, together with the recommended source in an SR instance. This allows the transforming application to "pull" the relevant information from the SR to populate the CDA header.
Table C.3-1. CDA Header content from SR
CDA Business Name |
DICOM SR |
ImagingReport: DocType |
Concept Name Code Sequence (0040,A043) [of the root content item] |
ImagingReport: ContentTemplate |
|
ImagingReport: DocumentID |
|
ImagingReport: Title |
(121050,DCM,"EquivalentMeaningofConceptName")>ConceptCode |
|
Sequence(0040,A168)>CodeMeaning(0008,0104)ifpresent;otherwise |
|
Concept Name Code Sequence (0040,A043) > Code Meaning |
|
(0008,0104) [of the root content item]. |
ImagingReport: CreationTime |
ContentDate(0008,0023)+ContentTime(0008,0033)+TimezoneOffset |
|
From UTC (0008,0201) |
ImagingReport: Confidentiality |
|
ImagingReport: LanguageCode |
(121049, DCM, "Language of Content Item and Descendants") |
ImagingReport: SetId |
|
ImagingReport: VersionNumber |
|
ImagingReport: Patient:ID |
Patient ID (0010,0020) |
ImagingReport: Patient:IDIssuer |
Issuer of Patient ID Qualifiers Sequence (0010,0024) > Universal Entity |
|
ID (0040,0032) |
ImagingReport: Patient:Addr |
Patient's Address (0010,1040) |
ImagingReport: Patient:Tele |
Patient's Telephone Numbers (0010,2154) |
ImagingReport: Patient:Name |
Patient's Name (0010,0010) |
ImagingReport: Patient:Gender |
Patient's Sex (0010,0040) |
|
[Map value "O" to nullFlavor UNK] |
ImagingReport: Patient:BirthTime |
Patient's Birth Date (0010,0030) + Patient's Birth Time (0010,0032) |
ImagingReport: Patient:ProviderOrgName |
Issuer of Patient ID (0010,0021) |
ImagingReport: Patient:ProviderOrgTel |
|
ImagingReport: Patient:ProviderOrgAddr |
|
ImagingReport: SigningTime |
Verifying Observer Sequence (0040,A073) > Verification DateTime |
|
(0040,A030). |
ImagingReport: SignerID |
Verifying Observer Sequence (0040,A073) > Verifying Observer |
|
Identification Code Sequence (0040,A088) [code value as identifier] |
ImagingReport: SignerAddr |
|
ImagingReport: SignerTel |
|
ImagingReport: SignerName |
Verifying Observer Sequence (0040,A073) > Verifying Observer Name |
|
(0040,A075) |
- Standard -
Page 124 |
DICOM PS3.20 2020a - Imaging Reports using HL7 Clinical Document Architecture |
|
|
CDA Business Name |
DICOM SR |
ImagingReport: SignatureBlock |
|
|
ImagingReport: Author:AuthoringTime |
ContentDate(0008,0023)+ContentTime(0008,0033)+TimezoneOffset |
|
|
|
From UTC (0008,0201) |
ImagingReport: Author:ID |
Author Observer Sequence (0040,A078) > Person Identification Code |
|
|
|
Sequence (0040,1101) [code value as identifier] |
ImagingReport: Author:Addr |
|
|
ImagingReport: Author:Tel |
|
|
ImagingReport: Author:Name |
Author Observer Sequence (0040,A078) > Person Name (0040,A123) |
|
ImagingReport: Recipient:Addr |
|
|
ImagingReport: Recipient:Tel |
|
|
ImagingReport: Recipient:Name |
|
|
ImagingReport: Recipient:Org |
|
|
ImagingReport: CustodianOrgID |
Custodial Organization Sequence (0040,A07C) > Institution Code |
|
|
|
Sequence (0008,0082) [code value as identifier] |
ImagingReport: CustodianOrgName |
Custodial Organization Sequence (0040,A07C) > Institution Name |
|
|
|
(0008,0080) |
ImagingReport: CustodianOrgAddr |
|
|
ImagingReport: CustodianOrgTel |
|
|
ImagingReport: EncounterID |
Admission Id (0038,0010) |
|
ImagingReport: EncounterIDIssuer |
Issuer of Admission ID Sequence (0038;0014) > Universal Entity ID |
|
|
|
(0040,0032) |
ImagingReport: EncounterTime |
|
|
ImagingReport: HealthcareFacilityName |
|
|
ImagingReport: HealthcareFacilityAddress |
Institution Address (0008,0081) |
|
ImagingReport:HealthcareProviderOrganizationName |
Institution Name (0008,0080) |
|
ImagingReport:AttendingPhysicianName |
Physician(s) of Record (0008,1048) |
|
ImagingReport:OrderPlacerNumber |
Referenced Request Sequence (0040,A370) > Placer Order |
|
|
|
Number/Imaging Service Request (0040,2016) |
ImagingReport:OrderAssigningAuthority |
Referenced Request Sequence (0040,A370) > Order Placer Identifier |
|
|
|
Sequence (0040,0026) > Universal Entity ID (0040,0032) |
ImagingReport:AccessionNumber |
Accession Number (0008,0050) |
|
ImagingReport:AccessionAssigningAuthority |
Issuer of Accession Number Sequence (0008,0051) > Universal Entity |
|
|
|
ID (0040,0032) |
ImagingReport:OrderedProcedureCode |
Referenced Request Sequence (0040,A370) > Requested Procedure |
|
|
|
Code Sequence (0032,1064) |
ImagingReport: OrderPriority |
|
|
ImagingReport:Study:StudyUID |
Study Instance UID (0020,000D) |
|
ImagingReport:Study:ProcedureCode |
Procedure Code Sequence (0008,1032) |
|
ImagingReport:Study:Modality |
(122142, DCM, "Acquisition Device Type") or (55111-9, LN, "Current |
|
|
|
Procedure Descriptions") > (122142, DCM, "Acquisition Device Type") |
ImagingReport:Study:AnatomicRegionCode |
(123014, DCM, "Target Region") or (55111-9, LN, "Current Procedure |
|
|
|
Descriptions") > (123014, DCM, "Target Region") |
ImagingReport:Study:StudyTime |
Study Date (0008,0020) + Study Time (0008,0030) + Timezone Offset |
|
|
|
From UTC (0008,0201) |
 ImagingReport: Performer:Type
ImagingReport: Performer:Type
- Standard -
DICOM PS3.20 2020a - Imaging Reports using HL7 Clinical Document Architecture |
Page 125 |
|
CDA Business Name |
DICOM SR |
|
ImagingReport: Performer:ID |
|
|
ImagingReport: Performer:Name |
|
|
ImagingReport: ReferrerAddr |
Referring Physician Identification Sequence (0008,0096) > Person's |
|
|
Address (0040,1102) |
|
ImagingReport: ReferrerTel |
Referring Physician Identification Sequence (0008,0096) > Person's |
|
|
Telephone Numbers (0040,1103) |
|
ImagingReport: ReferrerName |
Referring Physician's Name (0008,0090) |
|
ImagingReport: TranscriptionistID |
ParticipantSequence(0040,A07A)>PersonIdentificationCodeSequence |
|
|
(0040,1101),[whereParticipationType(0040,A080)equals"ENT"(Data |
|
|
Enterer); code value as identifier] |
|
ImagingReport: TranscriptionistName |
Participant Sequence (0040,A07A) Person Name (0040,A123) [where |
|
|
Participation Type (0040,A080) equals "ENT" (Data Enterer) ] |
|
ImagingReport: TransformedDocumentID |
SOP Instance UID (0008,0018) |
|
ImagingReport:Study:ModalityandImagingReport:Study:AnatomicRegionCodemaybemappedfromattributesintherootCONTAINER, if present there as in TID 2000, or in the Current Procedure Descriptions section CONTAINER, if present there as in TID 2006.
C.4 Body Transformation
For transformation of the body, this Section maps the SR content items to their target CDA elements. This allows the transforming application to traverse the SR content tree and construct equivalent CDA content.
C.4.1 Section Mapping
SR TID 2000, TID 2005 and TID 2006 specify that imaging report elements are contained in sections, represented as CONTAINERs with concept name codes from CID 7001.
Each CONTAINER immediately subsidiary to the root CONTAINER shall be mapped to the section or subsection as specified in Table C.4-1. Note that some SR document sections are mapped to subsections under CDA Template 1.2.840.10008.9.1.
Table C.4-1. SR Section mapping to CDA
Coding SchemeCode Value |
Code Meaning |
Map to Template Section/Subsection |
||
Designator |
|
|
|
|
LN |
11329-0 |
History |
9.2 |
Clinical Information / 9.8.3 Medical (General) |
|
|
|
History |
|
LN |
55115-0 |
Request |
9.2 |
Clinical Information / 9.8.1 Request |
LN |
55111-9 |
Current Procedure Descriptions |
9.3 |
Imaging Procedure Description |
LN |
55114-3 |
Prior Procedure Descriptions |
9.4 |
Comparison Study |
LN |
18834-2 |
Previous Findings |
9.4 |
Comparison Study |
LN |
18782-3 |
Findings (Study Observation) |
9.5 |
Findings or 9.5 Findings / 9.8.8 Fetus Findings |
|
|
|
(see C.4.1.3) |
|
LN |
59776-5 |
Findings |
9.5 |
Findings or 9.5 Findings / 9.8.8 Fetus Findings |
|
|
|
(see C.4.1.3) |
|
LN |
19005-8 |
Impressions |
9.6 Impression |
|
LN |
18783-1 |
Recommendations |
9.6 Impression / 9.8.11 Recommendation |
|
LN |
55110-1 |
Conclusions |
9.6 Impression |
|
LN |
55107-7 |
Addendum |
9.7 Addendum |
|
LN |
18785-6 |
Indications for Procedure |
9.2ClinicalInformation/9.8.2ProcedureIndications |
|
LN |
55108-5 |
Patient Presentation |
9.2 |
Clinical Information |
- Standard -