Материал: part20
Page 76 |
DICOM PS3.20 2020a - Imaging Reports using HL7 Clinical Document Architecture |
|
|
> |
0..1 |
MAY |
9.1.2 General |
|
|
|
Section Entries |
|
|
|
1.2.840.10008.9.23 |
9.8.1.1 text/content and @ID – CDS Record
The Request section narrative text block MAY include content blocks recording clinical decision support assessments of the request with respect to the indications, patient characteristics, and relevant guidelines. Each such text/content SHALL include an XML ID at- tribute that serves as the business name discriminator associated with an instantiation of the element. Even if only one content block is instantiated, the ID attribute shall be present.
Example 9.8.1.1-1. Request section example
<section classCode="DOCSECT" moodCode="EVN"> <templateId root="1.2.840.10008.9.7" />
<id root="1.2.840.10213.2.62.7906994785528.114289506"/> <code code="55115-0"
codeSystem="2.16.840.1.113883.6.1"
codeSystemName="LOINC" displayName="Request" />
<title>Request</title>
<text>PTA (Iliac Angioplasty) for treatment of symptomatic atherosclerotic disease in both iliac arteries.
<content ID="CDS001">Procedure ordered by Pat Smith, MD, NPI:8740944987. Classified APPROPRIATE by RadCDS based on ACR Select criteria
at 2015-07-21 10:52:31 CDT</content> </text>
</section>
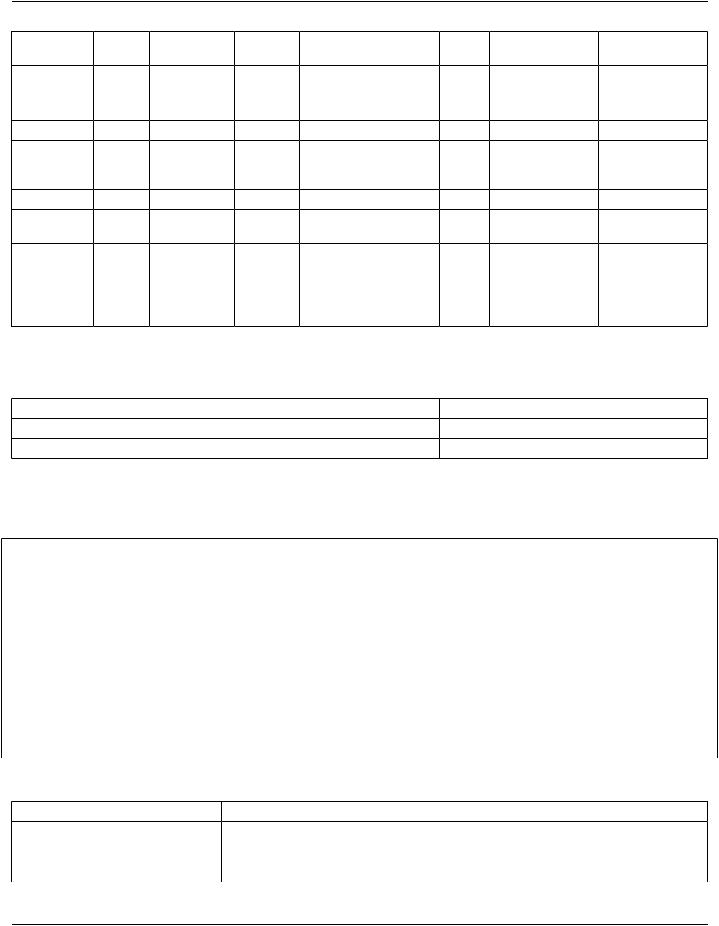
9.8.2 Procedure Indications
Template ID |
|
|
2.16.840.1.113883.10.20.22.2.29 |
|
|
|
Name |
|
|
Procedure Indications |
|
|
|
Effective Date |
|
|
2012-07 |
|
|
|
Version Label |
|
|
DICOM-20150324 |
|
|
|
Status |
|
|
Active |
|
|
|
Description |
|
|
Records details about the reason for the procedure. This section may include the |
|||
|
|
|
pre-procedure diagnosis or diagnoses as well as one or more symptoms that |
|||
|
|
|
contribute to the reason the procedure is being performed. |
|
||
Classification |
|
|
CDA Section Level |
|
|
|
Relationships |
|
|
Included in 9.2 Clinical Information |
|
|
|
Context |
|
|
parent node |
|
|
|
Open/Closed |
|
|
Open |
|
|
|
Revision History |
|
From Consolidated CDA r1.1 |
|
|
|
|
|
|
|
DICOM-20150324: adapted to use optional Coded Observation entry rather than |
|||
|
|
|
optional Indication entry |
|
|
|
Business |
Nest |
Element/ |
Card Elem/AttrConf Data |
Value |
Value |
Subsidiary |
Name |
Level |
Attribute |
Type |
Conf |
|
Template |
- Standard -
|
|
DICOM PS3.20 2020a - Imaging Reports using HL7 Clinical Document Architecture |
Page 77 |
||||
Procedure |
|
section |
1..1 |
SHALL |
|
|
|
Indications |
|
|
|
|
|
|
|
|
> |
templateId |
1..1 |
SHALL |
II |
|
|
|
>@ |
@root |
1..1 |
SHALL |
UID |
SHALL2.16.840.1.113883. |
|
|
|
|
|
|
|
10.20.22.2.29 |
|
|
> |
id |
1..* |
SHALL |
II |
|
|
|
> |
code |
1..1 |
SHALL |
CD |
SHALL(59768-2, LOINC, |
|
|
|
|
|
|
|
"Procedure |
|
|
|
|
|
|
|
Indications") |
|
Title |
> |
title |
1..1 |
SHALL |
ST |
|
|
Text |
> |
text |
1..1 |
COND |
ED |
|
9.1.1 Section Text |
|
|
|
|
|
|
|
1.2.840.10008.9.19 |
|
> |
entry |
0..* |
MAY |
|
|
|
Coded |
>> |
observation |
1..1 |
SHALL |
|
See 9.8.2.1 |
10.1 Coded |
Observation[*] |
|
|
|
|
entry/observation Observation |
||
|
|
|
|
|
|
|
2.16.840.1.113883. |
|
|
|
|
|
|
|
10.20.6.2.13 |
9.8.2.1 entry/observation
The binding to the Coded Observation concept domains is:
Concept Domain or Element |
Value Conf |
Value |
ObservationType |
SHOULD |
(432678004,SNOMED,"Indicationforprocedure") |
Other concept domains |
|
unspecified |
Note |
|
|
In Consolidated CDA r1.1 the binding to the observationType is to Value Set Problem Type (2.16.840.1.113883.3.88.12.3221.7.2) with conformance SHOULD. Values from that Value Set are acceptable here as well.
Example 9.8.2.1-1. Procedure indications section example
<section classCode="DOCSECT" moodCode="EVN"> <templateId root="2.16.840.1.113883.10.20.22.2.29"/> <id root="1.2.840.10213.2.62.044785528.1142895426"/> <code code="59768-2"
codeSystem="2.16.840.1.113883.6.1"
codeSystemName="LOINC" displayName="Procedure Indications"/>
<title>Procedure Indications</title>
<text>The procedure is performed as a follow-up for abnormal screening result.</text> </section>
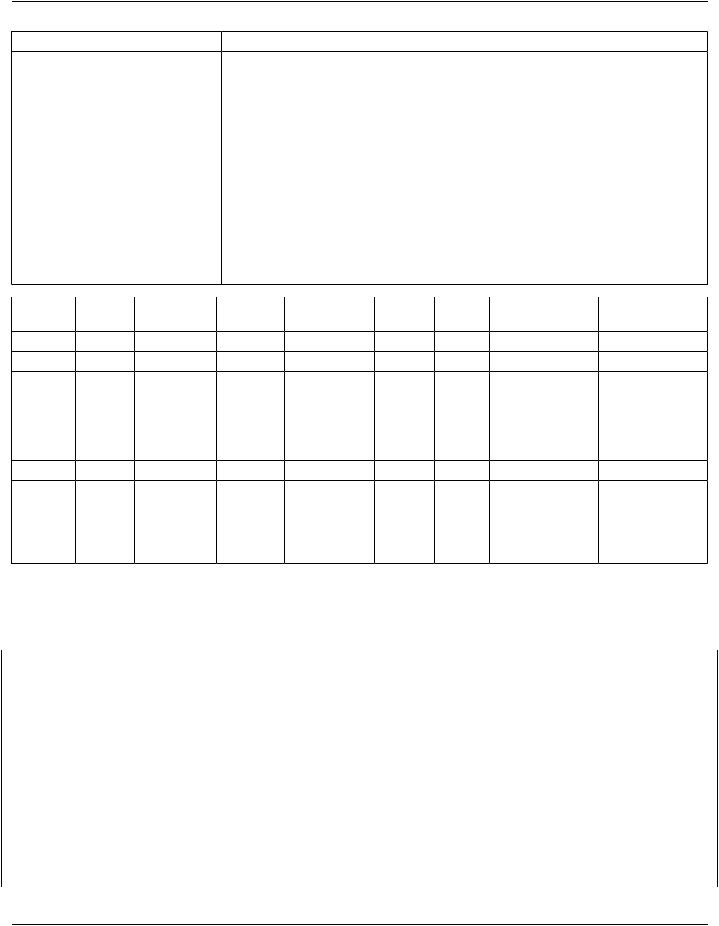
9.8.3 Medical (General) History
Template ID |
2.16.840.1.113883.10.20.22.2.39 |
Name |
Medical (General) History |
Effective Date |
2012-07 |
Version Label |
DICOM-20150324 |
- Standard -
Page 78 |
|
DICOM PS3.20 2020a - Imaging Reports using HL7 Clinical Document Architecture |
|
|||||
Status |
|
|
Active |
|
|
|
|
|
Description |
|
History general describes all aspects of medical history of the patient even if not pertinent |
||||||
|
|
|
tothecurrentprocedure,andmayincludechiefcomplaint,pastmedicalhistory,socialhistory, |
|||||
|
|
|
familyhistory,surgicalorprocedurehistory,medicationhistory,andotherhistoryinformation. |
|||||
|
|
|
The history may be limited to information pertinent to the current procedure or may be more |
|||||
|
|
|
comprehensive. It may also be reported as a collection of random clinical statements or it |
|||||
|
|
|
may be reported categorically. Categorical report formats may be divided into multiple |
|||||
|
|
|
subsections, including Past Medical History and Social History. |
|
||||
Classification |
|
CDA Section Level |
|
|
|
|
||
Relationships |
|
Included in 9.2 Clinical Information |
|
|
|
|||
Context |
|
|
parent node |
|
|
|
|
|
Open/Closed |
|
Open |
|
|
|
|
|
|
Revision History |
|
From Consolidated CDA r1.1 |
|
|
|
|||
|
|
|
DICOM-20150324: Addition of optional entries; C-CDA templateID retained |
|||||
Business Nest |
Element/ |
Card |
Elem/Attr Conf Data |
Value |
Value |
Subsidiary |
||
Name |
Level |
Attribute |
|
|
Type |
Conf |
|
Template |
History |
|
section |
1..1 |
SHALL |
|
|
|
|
|
> |
templateId |
1..1 |
SHALL |
II |
|
|
|
|
>@ |
@root |
1..1 |
SHALL |
UID |
SHALL 2.16.840.1.113883. |
||
|
|
|
|
|
|
|
10.20.22.2.39 |
|
|
> |
id |
1..* |
SHALL |
II |
|
|
|
|
> |
code |
1..1 |
SHALL |
CD |
SHALL (11329-0, LOINC, |
|
|
|
|
|
|
|
|
|
"History General") |
|
Title |
> |
title |
1..1 |
SHALL |
ST |
|
|
|
Text |
> |
text |
1..1 |
COND |
ED |
|
|
9.1.1 Section Text |
|
|
|
|
|
|
|
|
1.2.840.10008.9.19 |
|
> |
|
0..1 |
MAY |
|
|
|
9.1.2 General |
|
|
|
|
|
|
|
|
Section Entries |
|
|
|
|
|
|
|
|
1.2.840.10008.9.23 |
9.8.3.1 section/text
In the context of an Imaging Report, the section/text should document any contraindications to contrast administration or other pro- cedure techniques that affected the selection or performance of the protocol.
Example 9.8.3.1-1. Medical (General) History section example
<section classCode="DOCSECT" moodCode="EVN"> <templateId root="2.16.840.1.113883.10.20.22.2.39"/> <id root="1.2.840.10213.2.62.7044785528.114289875"/> <code code="11329-0"
codeSystem="2.16.840.1.113883.6.1"
codeSystemName="LOINC" displayName="History General"/>
<title>Relevant Medical History</title> <text>
<list>
<item>Patient reported adverse reaction to iodine.</item> <item>Patient is smoker (1 pack daily).</item>
- Standard -
|
DICOM PS3.20 2020a - Imaging Reports using HL7 Clinical Document Architecture |
Page 79 |
||||||
</list> |
|
|
|
|
|
|
|
|
</text> |
|
|
|
|
|
|
|
|
</section> |
|
|
|
|
|
|
|
|
9.8.4 Complications |
|
|
|
|
|
|
||
Template ID |
|
|
2.16.840.1.113883.10.20.22.2.37 |
|
|
|||
Name |
|
|
Complications |
|
|
|
|
|
Effective Date |
|
2012-07 |
|
|
|
|
||
Version Label |
|
DICOM-20150324 |
|
|
|
|||
Status |
|
|
Active |
|
|
|
|
|
Description |
|
|
The Complications section records problems that occurred during the procedure |
|||||
|
|
|
or other activity. The complications may have been known risks or unanticipated |
|||||
|
|
|
problems. |
|
|
|
|
|
Classification |
|
CDA Section Level |
|
|
|
|||
Relationships |
|
Included in 9.3 Imaging Procedure Description |
|
|||||
Context |
|
|
parent node |
|
|
|
|
|
Open/Closed |
|
|
Open |
|
|
|
|
|
Revision History |
|
From Consolidated CDA r1.1 |
|
|
||||
|
|
|
DICOM-20150324: Addition of optional entries |
|
||||
Business |
Nest |
Element/ |
Card |
Elem/Attr |
Data |
Value |
Value |
Subsidiary |
Name |
Level |
Attribute |
|
Conf |
Type |
Conf |
|
Template |
Complications |
section |
1..1 |
SHALL |
|
|
|
|
|
|
> |
templateId |
1..1 |
SHALL |
II |
|
|
|
|
>@ |
@root |
1..1 |
SHALL |
UID |
SHALL2.16.840.1.113883. |
||
|
|
|
|
|
|
|
10.20.22.2.37 |
|
|
> |
id |
1..* |
SHALL |
II |
|
|
|
|
> |
code |
1..1 |
SHALL |
CD |
SHALL(55109-3, LOINC, |
|
|
|
|
|
|
|
|
|
"Complications") |
|
Title |
> |
title |
1..1 |
SHALL |
ST |
|
|
|
Text |
> |
text |
1..1 |
COND |
ED |
|
|
9.1.1 Section Text |
|
|
|
|
|
|
|
|
1.2.840.10008.9.19 |
|
> |
entry |
0..* |
MAY |
|
|
|
|
Coded |
>> |
observation |
|
|
|
|
|
10.1 Coded |
Observation[*] |
|
|
|
|
|
|
|
Observation |
|
|
|
|
|
|
|
|
2.16.840.1.113883. |
|
|
|
|
|
|
|
|
10.20.6.2.13 |
Example 9.8.4-1. Complications section example
<section classCode="DOCSECT" moodCode="EVN"> <templateId root="2.16.840.1.113883.10.20.22.2.37"/>
<id root="1.2.840.10213.2.62.70444786655528.11428987524546666"/> <code code="55109-3"
codeSystem="2.16.840.1.113883.6.1"
- Standard -
Page 80 |
DICOM PS3.20 2020a - Imaging Reports using HL7 Clinical Document Architecture |
codeSystemName="LOINC"
displayName="Complications"/>
<title>Complications</title>
<text>Immediately following IV contrast injection, the patient reporting itching "all over". Dr. Smith examined the patient and found multiple urticaria. The patient denied difficulty breathing or swallowing. The patient was given Benadryl 50 mg PO and was followed for
30 minutes, during which time the symptoms subsided.</text> <entry>
<observation classCode="OBS" moodCode="EVN"> <templateId root="2.16.840.1.113883.10.20.6.2.13"/> <!-- Coded Observation -->
...
</observation>
</entry>
</section>
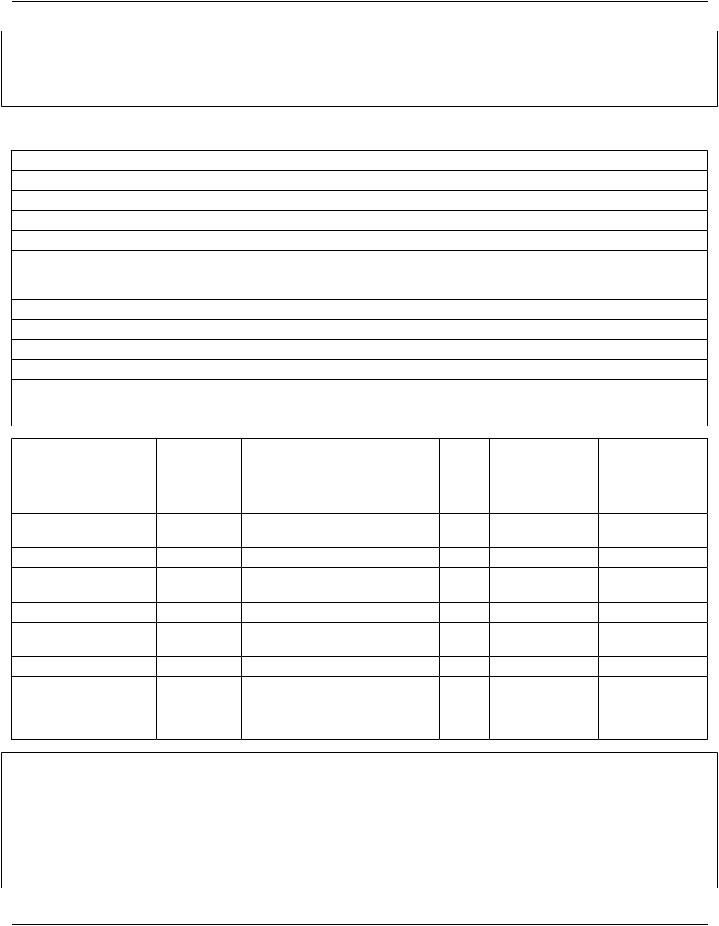
9.8.5 Radiation Exposure and Protection Information
Template ID |
1.2.840.10008.9.8 |
Name |
Radiation Exposure and Protection Information |
Effective Date |
2015/03/24 |
Version Label |
DICOM-20150324 |
Status |
Active |
Description |
Contains information related to the radiation exposure and protection of the |
|
patient, as may be required by national or local legal requirements or standards. |
Classification |
CDA Section and Entry Level |
Relationships |
Included in 9.3 Imaging Procedure Description |
Context |
parent node |
Open/Closed |
Open |
Revision History |
DICOM-20150324: Initial version |
Business |
Nest |
Element/ |
Card |
Elem/AttrData Value |
Value |
Subsidiary |
|
Name |
Level |
Attribute |
|
Conf |
Type Conf |
|
Template |
Radiation |
|
section |
1..1 |
SHALL |
|
|
|
Exposure |
|
|
|
|
|
|
|
|
> |
templateId |
1..1 |
SHALL |
II |
|
|
|
>>@ |
@root |
1..1 |
SHALL |
UID SHALL 1.2.840.10008.9.8 |
|
|
|
> |
code |
1..1 |
SHALL |
CD SHALL (73569-6, LOINC, |
|
|
|
|
|
|
|
|
"Radiation exposure and |
|
|
|
|
|
|
|
protection information") |
|
|
> |
id |
1..1 |
SHALL |
II |
|
|
Title |
> |
title |
1..1 |
SHALL |
ST |
|
|
Text |
> |
text |
1..1 |
SHALL |
ED |
|
9.1.1 Section Text |
|
|
|
|
|
|
|
1.2.840.10008.9.19 |
|
> |
entry |
0..1 |
COND |
|
|
|
|
>> |
procedure |
1..1 |
SHALL |
|
|
|
|
>>@ |
@classCode 1..1 |
SHALL |
CS SHALL PROC |
|
||
|
>>@ |
@moodCode1..1 |
SHALL |
CS SHALL EVN |
|
||
- Standard -