Материал: General propedeutics of internal diseases_Nemtsov-LM_2016
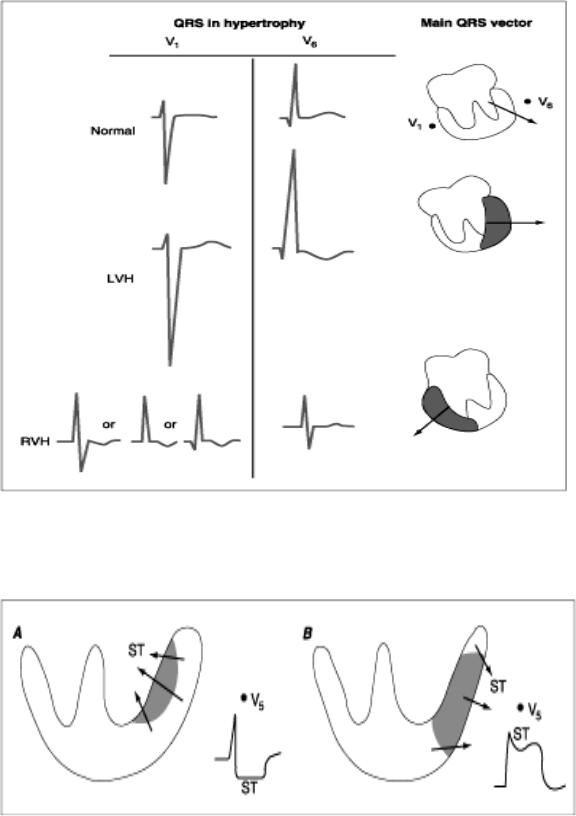
Fig. Suppl. 7. ECG in hypertrophy of ventricles.
Left-ventricular hypertrophy (LVH) - amplitude of the S increases in V1-2; amplitude of the R increases >20-25 mm in V4-6.
Right-ventricular hypertrophy (RVH) the changes in the S and R waves are the reverse - high R wave ≥ 7 mm in V1-2, deep S wave in V4-6 .
Fig. Suppl. 8. Acute ischemia causes a current of injury of myocardium.
Subendocardial injury (A) - the resultant ST vector directs toward the inner layer of the affected ventricle, overlying leads therefore will record ST depression. Transmural or epicardial injury (B) - ST elevations and sometimes tall, positive, hyperacute T waves over the ischemic zone.
165
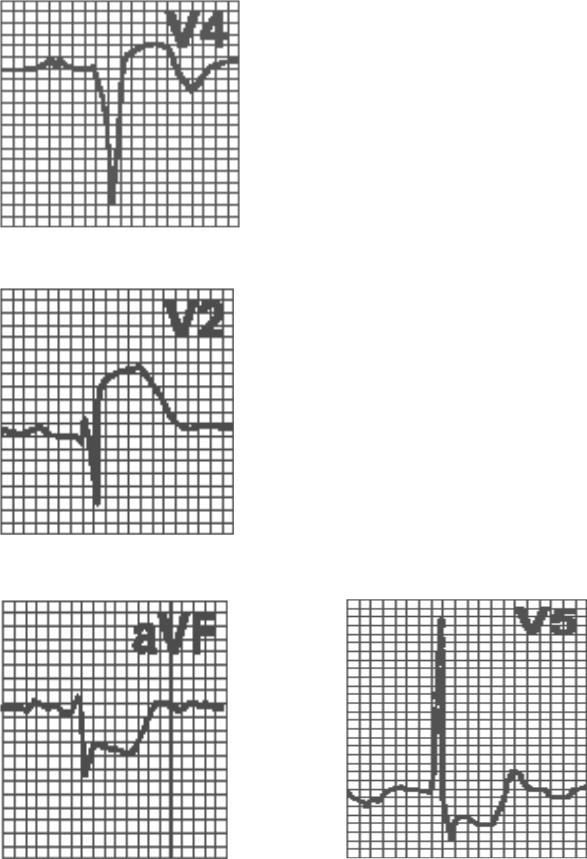
Fig. Suppl. 8. Myocardial necrosis is detected by the pathological Q-wave - - width≥0.04 s (in V4-6 >0.025 s), depth>2 mm or>1/4 R-wave (in V4-6 >15%R).
Fig. Suppl. 9a. Ischemic myocardium injury is detected by ST-interval.
Transmural or epicardial injury - convexing elevation ST with transmission in T- wave.
Fig. Suppl. 9b. Subendocardial injury – horisontal or concaving depression ST.
166
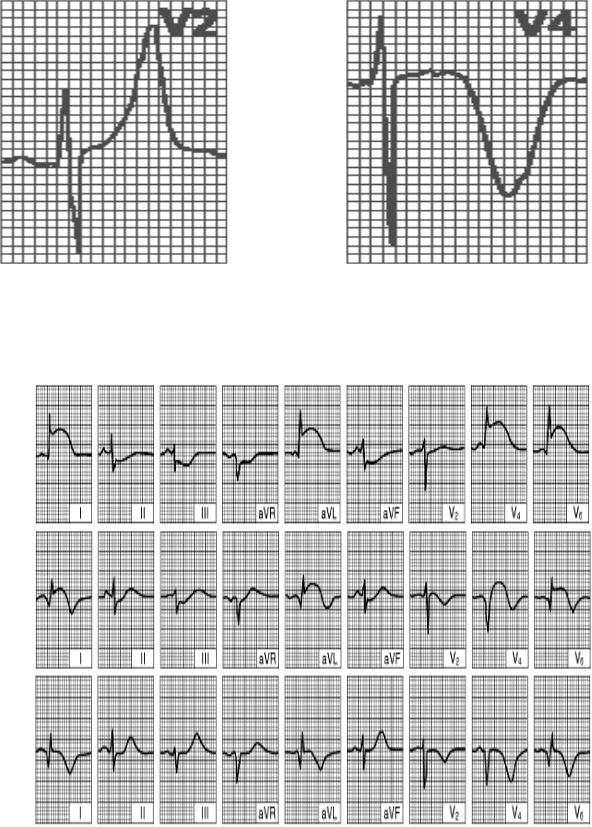
Fig. Suppl. 10. Ischemia of myocardium is detected by T-wave.
Subendocardial ischemia - symmetrical acute high T-wave in overlying leads (>6 mm in standard and augmented leads , >8-10 mm in chest leads)
Transmural or epicardial ischemia symmetrical acute deep T-wave.
A
B
C
Fig. Suppl. 11. Acute anterior left ventricular myocardial infarction
(A) Superacute period (1-2 hours), (B) acute period (24 hours), (C) subacute period (>1 week).
167
A
B
C
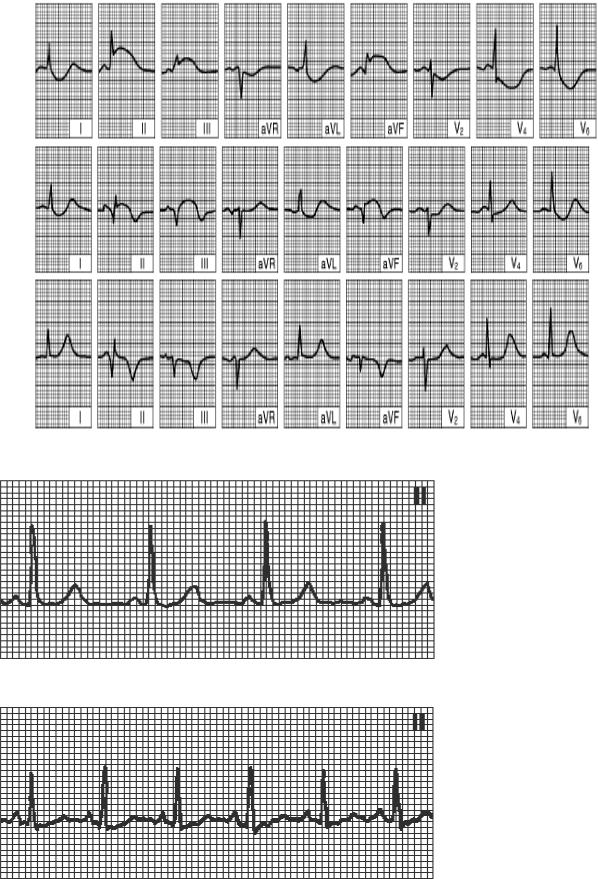
Fig. Suppl. 12. (A) Superacute period (1-2 hours), (B) acute period (24 hours),
(C) subacute period (>1 week).
Fig. Suppl. 13. Normal sinus rhythm.
HR=60-80 in min, P(+) I, II, aVF, (-) aVR, PQ ≥0,12s
Fig. Suppl. 14. Sinus tachycardia.
HR>90 in min, regular rhythm.
168
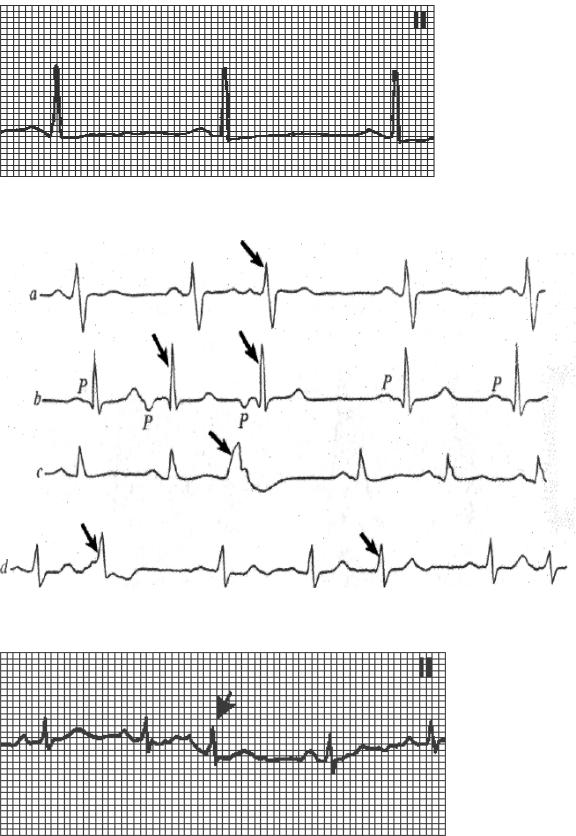
Fig. Suppl. 15. Sinus bradycardia.
HR<60 in min, regular rhythm.
Fig. Suppl. 16. Extrasystolic arrhythmia:
a – atrial extrasystole, b - AV-junction extrasystole, c – ventricular extrasystole ,d - polytopic extrasystole.
Fig. Suppl. 17. Atrial extrasystole: (1) premature appearance of the cardiac complex, (2) P wave - normal shape or slightly disfigured and superimposed on the preceding T wave; (3) normal shape of QRS (4) incomplete compensatory pause.
169